Session Information
Date: Sunday, October 26, 2025
Title: (0430–0469) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Treat-to-target is the guiding principle and therapeutic strategy for rheumatoid arthritis (RA) treatment. Escalation of treatment is based on the regular assessment of disease activity to attain and maintain an established target. Although remission is the preferred target of treatment, low disease activity (LDA (CDAI >2.8 and ≤10)) may be an acceptable target. It remains unclear if patients attaining LDA have incremental benefit after 1 to 2 years, if they can remain with a CDAI < 10. This study aims to evaluate differences in outcomes among patients with RA treated to LDA and then followed over a two-year period.
Methods: Data were collected from 522 adult patients in a private practice with established RA treated with advanced therapies, who completed a questionnaire at every visit and were evaluated with a physical exam. Those who attained LDA at baseline and remained with CDAI < 10 at 1 and 2 years were studied. Data included patient demographics, disease duration, smoking status, CDAI, DAS28, RAPID3, MDHAQ function (FN), pain VAS, patient global VAS (PtGlb), MDHAQ fatigue, joint replacements, depression, swollen joints, tender joints, physician global VAS (DocGlb), ESR and CRP. At Year 1 and 2, Remission was defined as CDAI < 2.8, Very Low Disease Activity (VLDA) was defined as CDAI ≥ 2.8 and ≤ 6, and High LDA (HLDA) was defined as CDAI > 6 and ≤ 10. Data were analyzed with two-sample T tests.
Results: 143 patients with established RA with low CDAI at baseline receiving DMARD therapy (CS-DMARD, B-DMARD, or TS-DMARD) were followed at 1 and 2 years. 47 (33%) patients achieved remission, 53 (37%) achieved VLDA, and 43 (30%) patients achieved HLDA at follow-up. Patients who achieved remission had improved documented global scores and MDHAQ function scores compared to patients in VLDA and HLDA at both 1 and 2 years (p< 0.05), and less damaged joints compared to patients in HLDA at 1 year (p< 0.05). Remission was not significant for less damaged joints compared to VLDA. There was no observable difference at 1 or 2 years in age, sex, duration of disease, self-reported joint replacements or depression scores between patients who achieved remission vs VLDA vs HLDA. Similarly, patients in VLDA did better than those in HLDA. At year 1: Swollen Count, Pain, PtGlb, Fatigue and RAPID3, and at Year 2: Swollen Count, DocGlb, Fn, Pain, PtGlb, Fatigue, DAS28-CRP and RAPID3 were all significantly better in VLDA vs. HLDA (p< 0.05).
Conclusion: Patients who successfully achieved remission from a baseline of low disease activity were found to have improved functional and clinical outcomes after 1 and 2 years. Patients who achieved VLDA had improvement but to a lesser degree. Finally, while remaining in LDA, patients in HLDA had worse outcomes compared to Remission or VLDA.
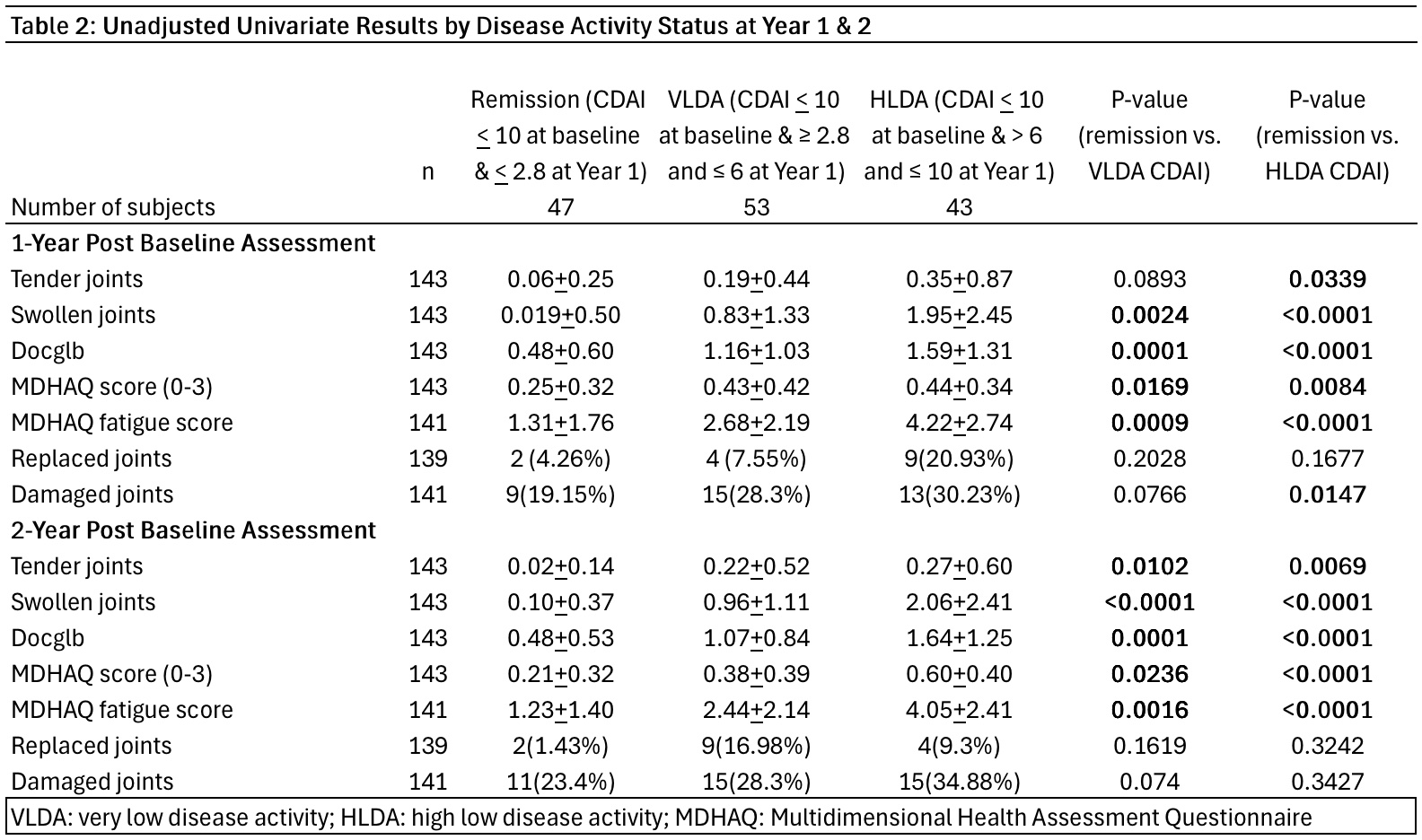 Table 1
Table 1
.jpg) Table 2
Table 2
To cite this abstract in AMA style:
Thoman E, Porcu S, Bergman M. Low Disease Activity: Good Enough? [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/low-disease-activity-good-enough/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-disease-activity-good-enough/