Session Information
Date: Sunday, October 26, 2025
Title: (0430–0469) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with rheumatic disease have an increased risk for thrombotic events and major adverse cardiac events (MACE) due to systemic inflammation. Bleeding time is a test performed in the clinic and consistently confirms a short time to clot with known risk factors such as estrogen, cox-2 inhibitors, JAK inhibitors, and factor V Leiden. Historically, a short bleeding time under 3 minutes is associated with an increased risk of thrombotic disease. We explored whether patients with rheumatic disease have a short bleeding time. This may be the physiologic mechanism leading to clotting events.
Methods: All sequential 239 patients over age 50 with rheumatic disease had a bleeding time test (BT). This included patients with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, and lupus. Data was collected between September 2022- December 2024. Patients who began low dose aspirin 81 mg daily in 2023 had a repeat BT to confirm compliance. No patients had a history of cardiovascular disease but 15 developed MACE or a thrombotic event prior to aspirin therapy, and this resulted in death for three patients. BT at baseline (prior to the event) and BT after the event were compared. Cohorts were analyzed by assigned treatments for rheumatic disease including methotrexate, JAK inhibitors, TNF inhibitors, abatacept, secukinumab, IL-1 inhibitors, and PD-1 agonist.
Results: Rheumatic disease patients at baseline had shorter BT results compared to historical normal controls (1.52 + 0.77) versus 4-7 minutes which is found in the normal general population (p< 0.01). There was no difference in the short BT among patients with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, or lupus. Cohorts were analyzed by treatment and BT did not discriminate between treatment assigned (Table 1). The addition of low dose aspirin 81 mg daily dramatically nearly doubled BT. The patients who developed MACE or a thrombotic event had short BT test results but did not differ from those who did not have a clotting event. The only significant findings in the MACE/thrombotic group was older age by almost a decade, predominantly male gender, and 80% were smokers (Table 2).
Conclusion: All patients with rheumatic disease with systemic inflammation tested had short BT results. BT did not identify a specific individual who would develop MACE or a thrombotic event. BT tests did revert to normal with the addition of low dose aspirin 81 mg daily. Aspirin is now recommended prophylactically in all lupus with phospholipid syndrome. Perhaps it is time to consider low dose aspirin for patients over age 50 with rheumatic disease.
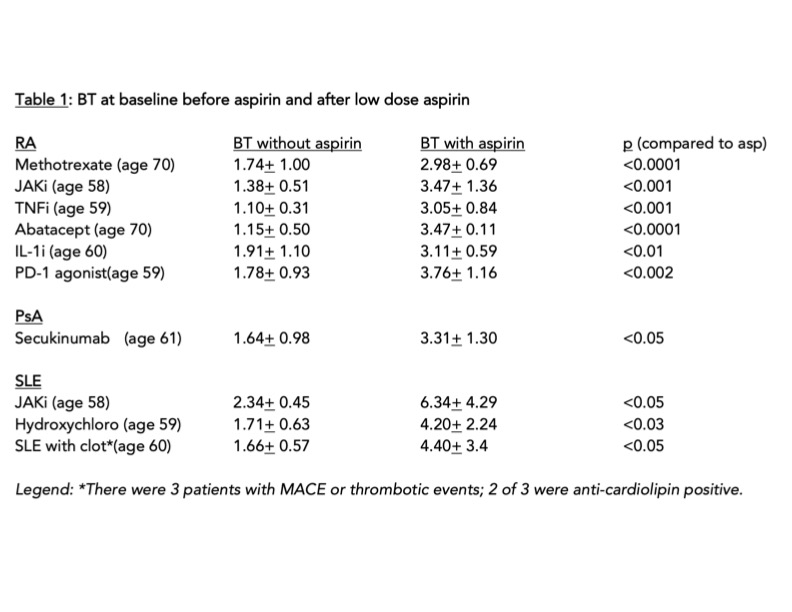 Table 1
Table 1
.jpg) Table 2
Table 2
To cite this abstract in AMA style:
Mazariego A, Greenwald M. Why Do Patients with Rheumatic Disease Have MACE and Thrombotic Events? [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/why-do-patients-with-rheumatic-disease-have-mace-and-thrombotic-events/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/why-do-patients-with-rheumatic-disease-have-mace-and-thrombotic-events/