Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Immune checkpoint inhibitor-induced inflammatory arthritis (ICI-IA) is an impactful and often persistent side effect of cancer immunotherapy that can lead to permanent joint damage and negatively affect quality of life. Though there are similarities between ICI-IA and other forms of inflammatory arthritis like rheumatoid arthritis (RA), key differences exist between these conditions. Patients with ICI-IA are commonly seronegative and are clinically heterogeneous in severity of arthritis, particular joints involved, presence of tendon and myofascial inflammation, and duration of arthritis symptoms. Importantly, patients with ICI-IA also have cancer and may experience additional side effects of cancer treatment. We evaluated symptoms and impacts in patients with ICI-IA and their correlation with arthritis disease activity.
Methods: Patients at Johns Hopkins with rheumatologist diagnosed ICI-IA and who filled out PRO questionnaires at baseline rheumatology visit were included. PROs measured with PROMIS short forms in both cohorts included physical function, ability to participate in social roles, pain interference, fatigue, anxiety, depression, and sleep disturbance. Disease activity was measured by clinical disease activity index (CDAI). For demographic, clinical, and PROMIS measures, summary statistics were calculated. Patients with ICI-IA only were then divided by CDAI categories, and PROMIS scores were compared with one way ANOVA and post hoc contrasts.
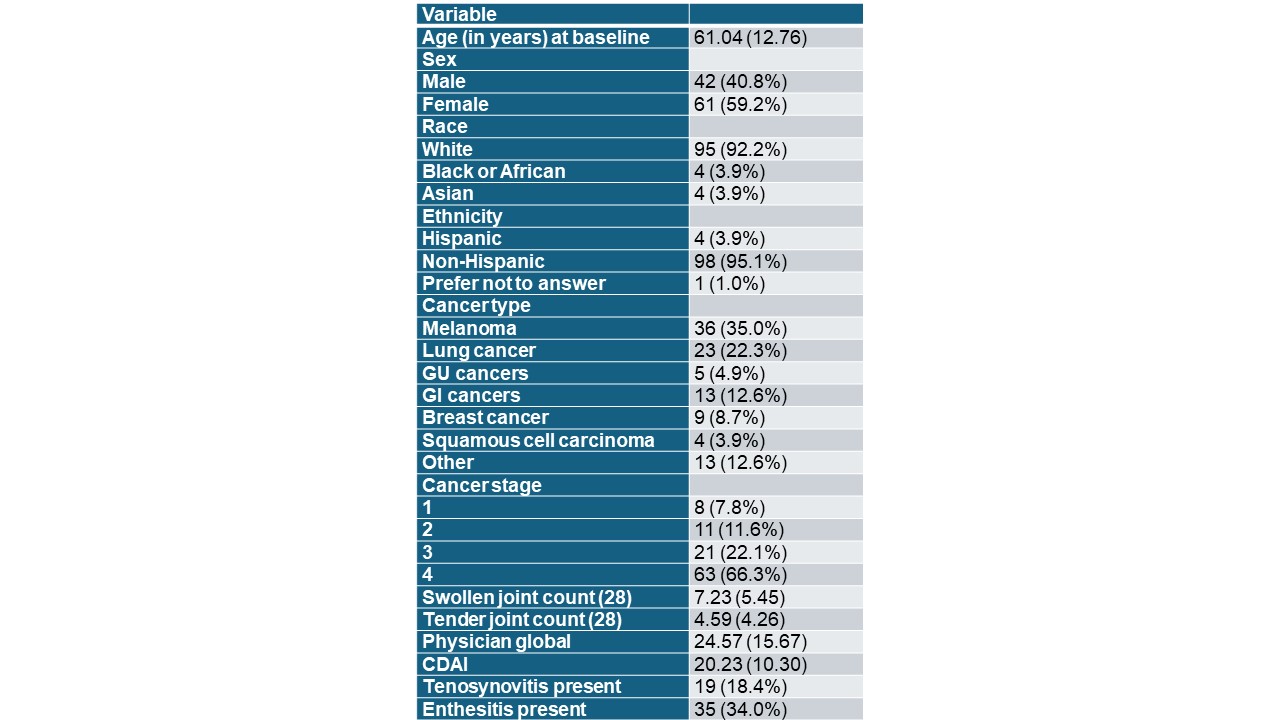
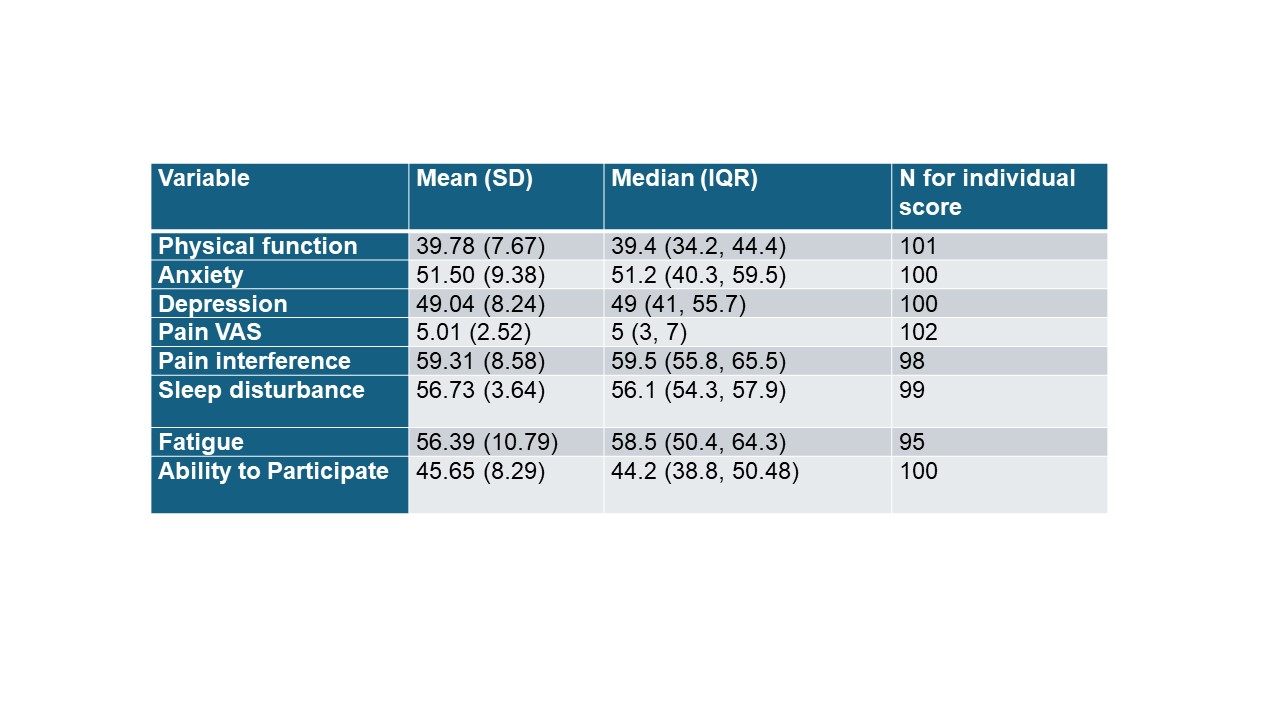
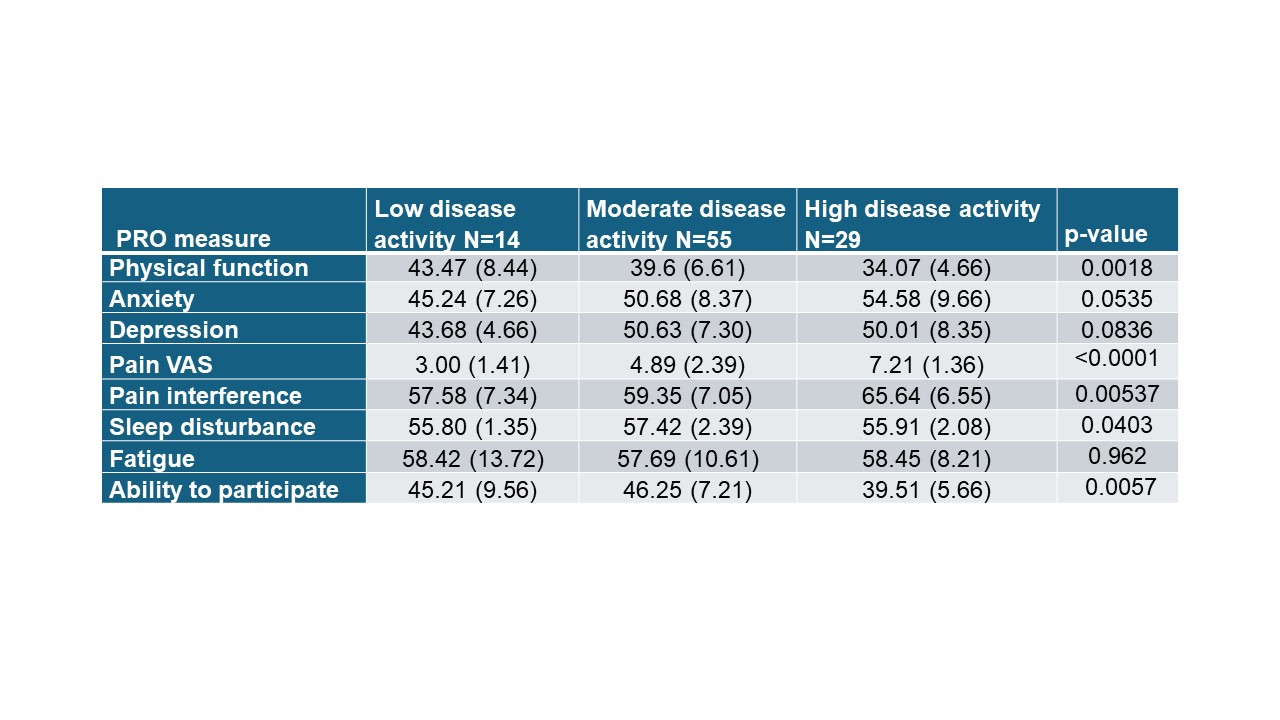
Results: 100 patients with ICI-IA were included. Patients with ICI-IA were 61 years old on average and more commonly female (59.2%). Melanoma was the most common cancer followed by lung cancer (Table 1). Average CDAI was 20.23 indicating a moderate disease activity (Table 1). Patients with ICI-IA had worsened levels of pain interference, fatigue, and physical function as compared to the population norm of 50, while anxiety and depression were close to population normative values (Table 2). When PROs were compared by CDAI category for ICI-IA, several were worse in patients with high disease activity as compared to those with low or moderate disease activity (Table 3). Specifically, pain interference was higher and the ability to participate and physical function were lower (worsened) in those with high disease activity. Interestingly fatigue was similarly increased compared to population norms regardless of IA disease activity.
Conclusion: Patients with ICI-IA have worsened pain interference, physical function, ability to participate, and fatigue compared to population normative values, while anxiety and depression were similar to the general population. Some of these symptoms and impacts increase with IA disease activity, but fatigue similarly affects patients with ICI-IA regardless of CDAI. These findings highlight the severity of impacts of ICI-IA on health-related quality of life, but also show that fatigue may be troublesome for patients with ICI-IA regardless of their arthritis disease activity.
To cite this abstract in AMA style:
Cappelli L, Eaton C, Wang Y, Jones M, Bingham C. Pain and Physical Function, but Not Fatigue, Track with Disease Activity in Immune Checkpoint Inhibitor-Induced Inflammatory Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/pain-and-physical-function-but-not-fatigue-track-with-disease-activity-in-immune-checkpoint-inhibitor-induced-inflammatory-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pain-and-physical-function-but-not-fatigue-track-with-disease-activity-in-immune-checkpoint-inhibitor-induced-inflammatory-arthritis/