Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: End-stage renal disease (ESRD) secondary to vasculitis is linked to a higher risk of vertebral fractures compared to other causes of ESRD. It remains unclear whether this association specifically applies to individuals on chronic dialysis who have granulomatosis with polyangiitis (GPA), in which corticosteroid dose or other clinical factors might mediate this relationship.
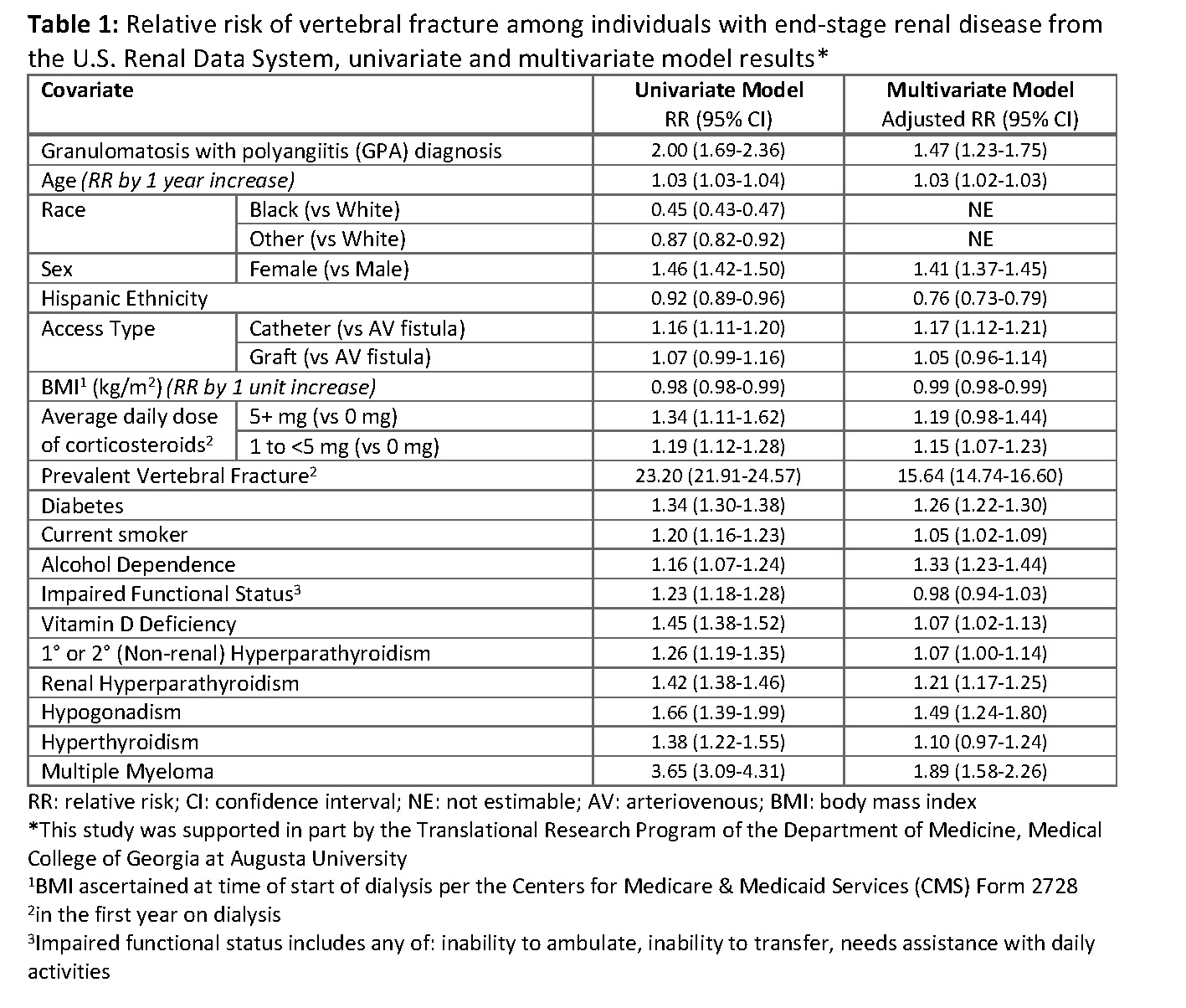
Methods: A retrospective cohort study was conducted using data from adults in the U.S. Renal Data System (USRDS), who began dialysis between 2006 and 2017, survived at least one year, and had continuous Medicare Part D coverage during the first year of dialysis. A person was considered to have GPA if there was an International Classification of Diseases (ICD)-9 or ICD-10 code for GPA (446.4, M31.30, or M31.31) in the one year following the start of dialysis. Incident vertebral fractures were defined by ICD-9/10 codes, requiring either one inpatient code or two outpatient codes within 90 days. Time at risk for vertebral fracture started one year after dialysis initiation and continued until the first incident vertebral fracture, death, or end of study period (12/31/2019). Multivariable logistic regression assessed the association of GPA with incident vertebral fracture among persons with ESRD, controlling for many clinically relevant covariates, including demographics, body mass index (BMI), dialysis factors, and impaired functional status from Centers for Medicare & Medicaid Services (CMS) Form 2728. We further adjusted for prevalent vertebral fracture, lifestyle-related factors, and other causes of metabolic bone disease from ICD-9/10 codes and corticosteroid average daily dose (0, 1 to < 5, or 5+ mg/day) from pharmacy claims data within the first year after dialysis start.
Results: There were 629,974 persons with ESRD included in our study: 46% women, 63% White, 31% Black, 15% Hispanic, and almost exclusively (99.96%) on hemodialysis. Most participants (96.4%) were not taking corticosteroids, but 3.3% were taking a daily prednisone-equivalent dose of 1 to < 5 mg/day and 0.4% were taking ≥ 5 mg/day. Among study participants, 2,204 (0.4%) had GPA. Vertebral fractures were observed in 155 individuals with GPA (7.0%) and 20,236 without GPA (3.2%). GPA was associated with a significantly increased risk of vertebral fracture (adjusted relative risk: 1.47, 95% confidence interval: 1.23-1.75) (Table 1).
Conclusion: Our findings suggest individuals with ESRD and GPA face a higher risk of vertebral fracture compared to persons with ESRD without GPA. Future studies examining specifically individuals with ESRD secondary to GPA are needed to augment these findings; our cohort included individuals with both ESRD and GPA, but we did not consider whether the ESRD was a direct result of vasculitis in GPA.
To cite this abstract in AMA style:
El Hajj J, Waller J, Patel Y, Bollag W, Baer S, Elam R. Risk of Vertebral Fracture in Individuals with Granulomatosis with Polyangiitis and End-Stage Renal Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/risk-of-vertebral-fracture-in-individuals-with-granulomatosis-with-polyangiitis-and-end-stage-renal-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-of-vertebral-fracture-in-individuals-with-granulomatosis-with-polyangiitis-and-end-stage-renal-disease/