Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Hand impairment is a prevalent issue among systemic sclerosis (SSc) patients and contributes to disability and diminished quality of life. Managing hand pain can be challenging due to the coexistence of various manifestations such as inflammatory arthritis, tendinopathies, joint contractures, sclerodactyly, calcinosis, acro-osteolysis, Raynaud’s phenomenon (RP), digital ulcers (DU), and chronic pain. The physical examination and radiographs are the primary methods for evaluating hand pain but are limited in scope. We hypothesized that joint ultrasound (US) is more sensitive than combined joint exam and hand radiograph for identification of acro-osteolysis, articular disease (synovitis, erosions, osteophytes), and periarticular disease (tendinopathies, calcinosis) and can assist in targeted treatment strategies.
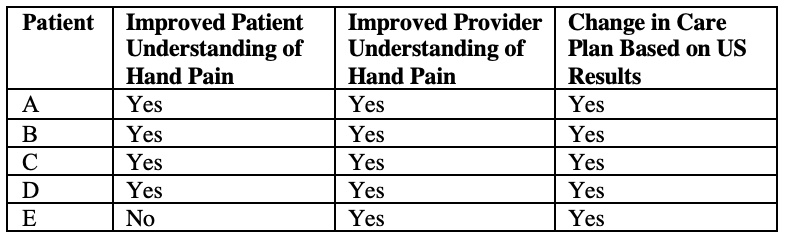
Methods: Five randomly selected SSc patients with nonspecific hand pain were referred for musculoskeletal US exam. SSc clinical features were recorded. Joint US was compared to physical exam features of synovitis, tendinopathy, digital ulcers, or calcinosis and radiographic features of erosions, osteophytes, and acro-osteolysis. A pre- and post-ultrasound survey assessed patient and provider perception of diagnostic understanding and treatment needs.
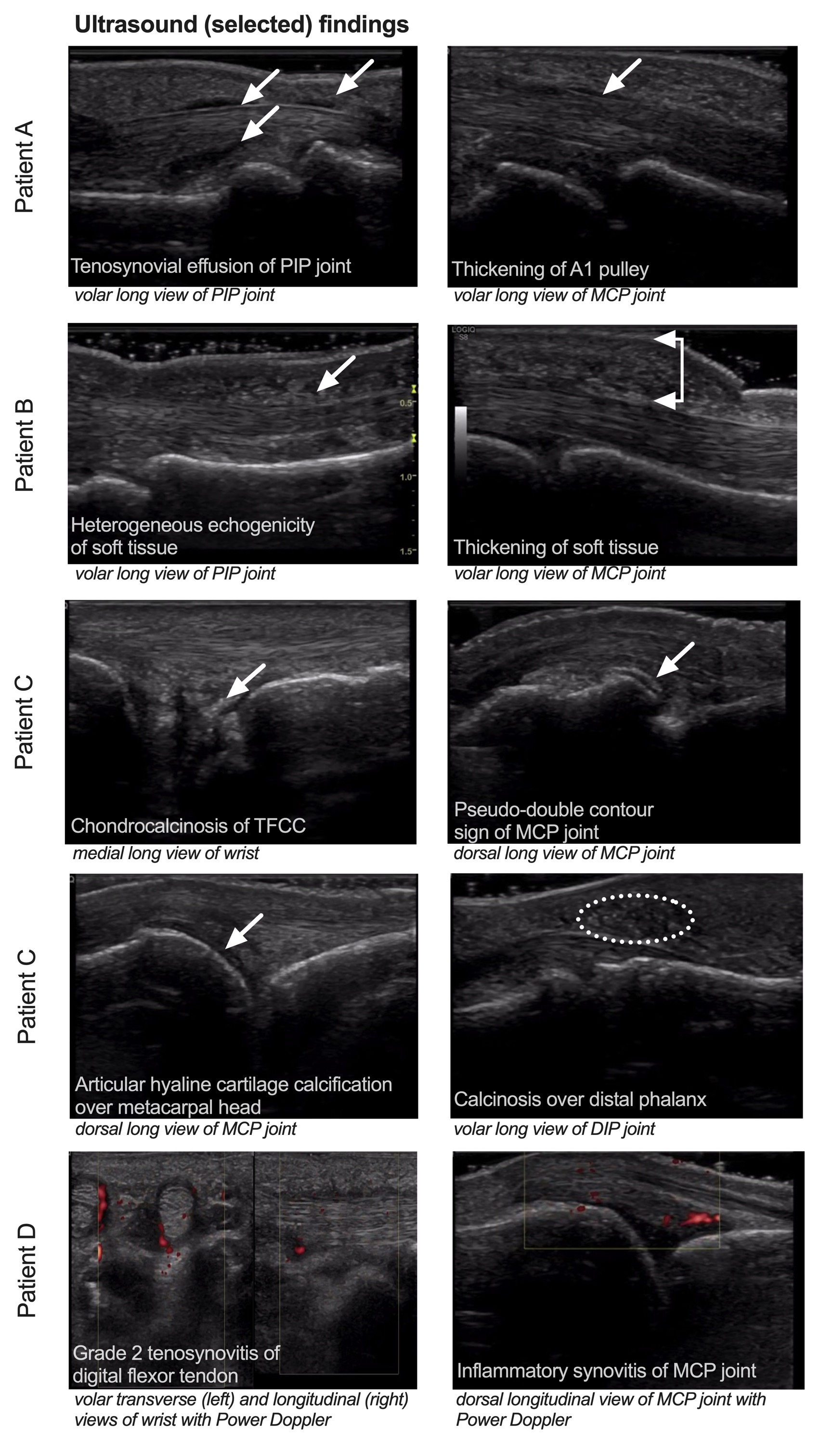
Results: Baseline characteristics, exam findings, radiographs, and ultrasound findings are noted in Table 1. No patients had digital ulcers or calcinosis on physical exam or acro-osteolysis on radiograph. Ultrasound exam was able to detect diverse manifestations of hand pathology (Figure 1). Ultrasound review improved the referring provider’s confidence in treatment decision improved in all cases (Table 2). Patient A was diagnosed with mechanical osteoarthritis, patient B with sclerodactyly, patient C with calcium pyrophosphate arthropathy, Patient D with inflammatory arthritis, and Patient E with chronic pain. The treatment plan was modified in all five patients. US improved patients’ understanding of the cause of their joint pain in four patients. After undergoing US, all patients reported feeling that their joint problem had been more thoroughly examined and being more likely to adhere to their provider’s treatment recommendations.
Conclusion: The physical exam and radiographs are not sufficient for the evaluation of hand pain in systemic sclerosis. Standardized US assessment in SSc can accurately evaluate hand pain and quantify acro-osteolysis, articular disease, and periarticular disease. Detection of these features can improve provider confidence in management decisions and advance patient understanding of disease, potentially improving treatment adherence and outcomes.
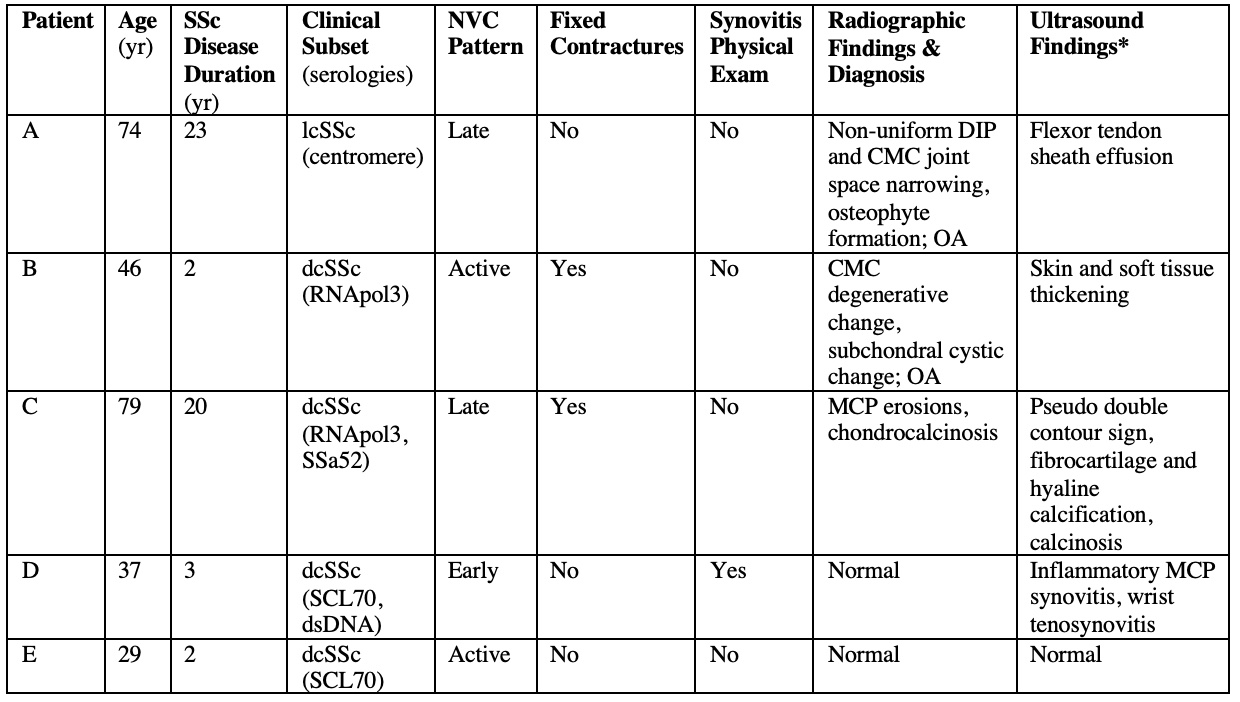
Yr= years; lcSSc= limited cutaneous systemic sclerosis; dcSSc= diffuse cutaneous systemic sclerosis; NVC= nailfold videocapillaroscopic pattern; DIP= distal interphalangeal; CMC= carpometacarpal; OA= osteoarthritis; MCP= metacarpophalangeal; CPPD= calcium pyrophosphate deposition.
*Summarized ultrasound findings are displayed in Table 1 with specific pathologic features detected on ultrasound represented in Figure 1.
PIP= proximal interphalangeal; MCP= metacarpophalangeal; TFCC= triangular fibrocartilage complex; DIP= distal interphalangeal
PIP= proximal interphalangeal; MCP= metacarpophalangeal; TFCC= triangular fibrocartilage complex; DIP= distal interphalangeal
To cite this abstract in AMA style:
Balbach M, Frech T, Chadwick N, Byram K, Chew E. Diagnostic and Educational Utility of an Ultrasound Protocol for Evaluation of Hand Pain in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/diagnostic-and-educational-utility-of-an-ultrasound-protocol-for-evaluation-of-hand-pain-in-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-and-educational-utility-of-an-ultrasound-protocol-for-evaluation-of-hand-pain-in-systemic-sclerosis/