Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Some of the most commonly reported side effects of statins (widely used lipid lowering agents) are muscle injury (incidence ranging from 0.1-20% based on type of muscle disorder) and hepatic dysfunction (incidence < 3%). Creatine kinase (CK) level in the blood is the most commonly used marker for assessing statin-induced myopathy. Apart from liver, skeletal muscles also produce transaminases. It is important to diagnose statin induced myopathy at an early stage in order to prevent complications such as rhabdomyolysis and immune mediated necrotizing myopathy. Continuing statins when there is muscle inflammation can lead to severe muscle weakness and disability. We explored how frequently clinicians check CK in patients with elevated transaminases to look for muscle injury.
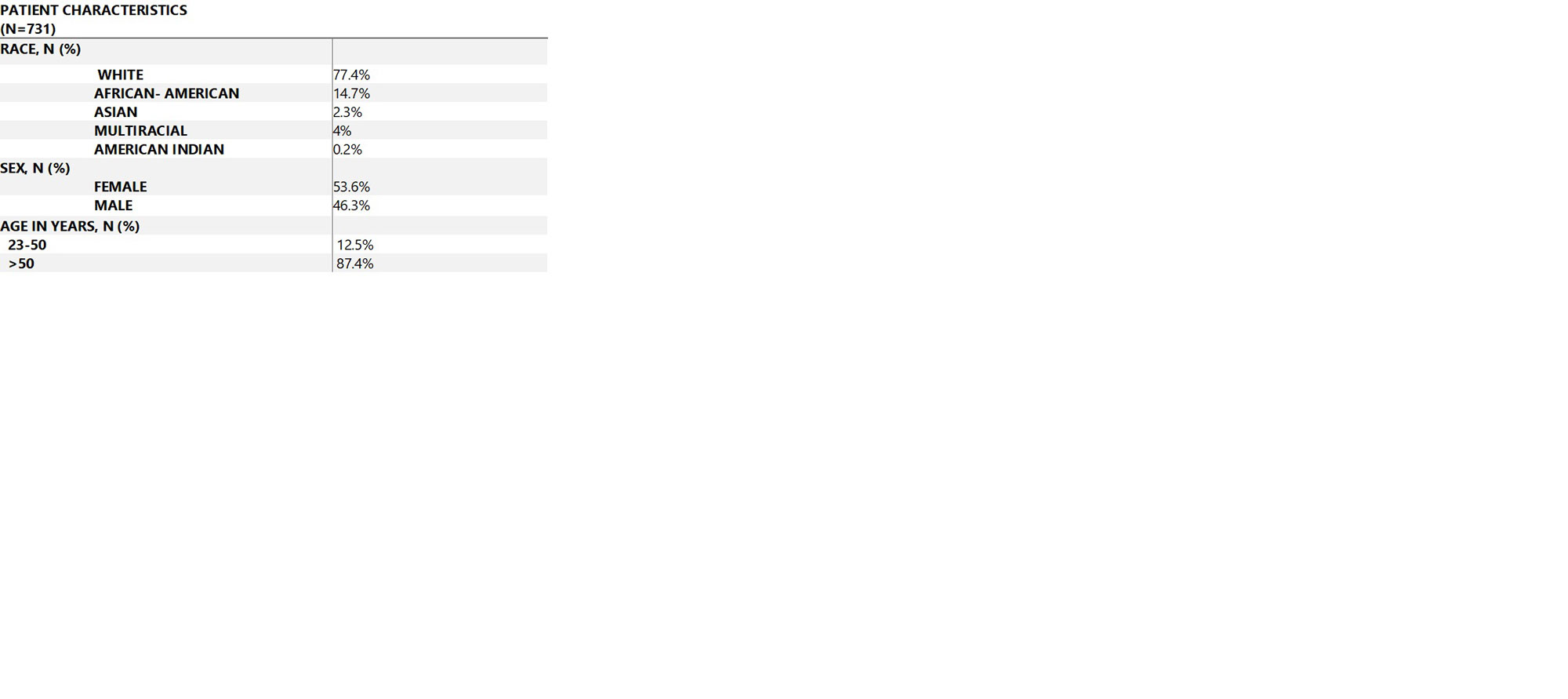
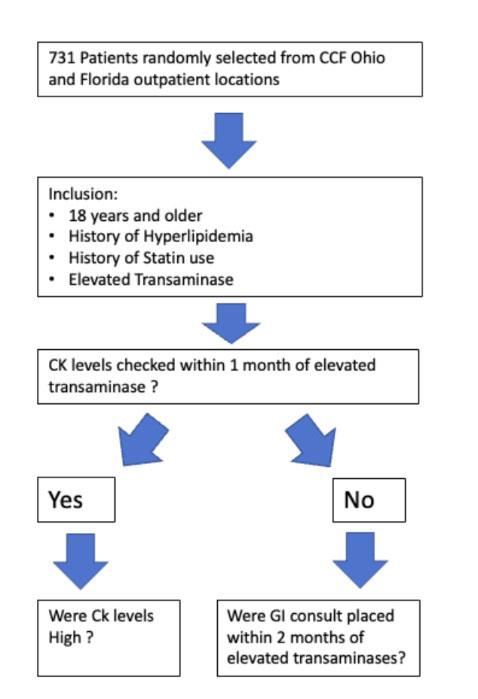
Methods: This was a quality improvement project done through a retrospective chart review conducted in the various outpatient departments of Cleveland Clinic, OH and FL over a period of 5 years, from May 2017 to May 2022. We randomly selected 731 patients in outpatient setting who were taking statins and were diagnosed with elevated transaminases using ICD code: R74.01. Then we reviewed the records to ascertain if the subjects had a CK level checked within 1 month of diagnosis of elevated transaminases. Only total CK was considered; CK isoenzyme levels were not. Records were also reviewed for patients who did not have their CK level checked within 1 month of the diagnosis but had a gastroenterology consult placed within 2 months of the diagnosis. We labelled CK as elevated when they were flagged high per the laboratory cut off value (which varied based on laboratory, sex and age).
Results: Among 731 patients, only 169, or 23 %, had their CK checked within one month of the ICD10 diagnosis of elevated transaminase. Of these 169 subjects, 26 patients, or 15 %, had CK flagged as high based on laboratory cut offs. Among these 26 patients, 65 % had CK level >400 U/L and 19 % had CK level >1000 U/L. Hence, 3.5 % of the total study population had elevated CK levels.
562 patients, or 77 % did not have their CK checked. Of those who did not have CK checked, 20 patients, or 3.5 % had a gastroenterology consult placed within 2 months of the ICD diagnosis for further liver status workup.
Conclusion: We found that in our clinic, the majority of patients on statins with elevated transaminase levels did not have their CK checked in a timely fashion. Finding an elevated CK may prevent further unnecessary testing of liver status, reduce healthcare costs and allow for earlier treatment of statin- induced muscle damage. Efforts to train physicians to check muscle enzymes in patients on statins should be undertaken. Electronic Medical Record system(EMR) flagging of elevated transaminase levels prompting a CK check could be implemented.
To cite this abstract in AMA style:
NIDHAAN A, Hastings A, gonzalez d, joshi r, gilbert n, o'connor c. Frequency of Checking Creatine Kinase in Patients on Statins with Elevated Transaminase for Early Detection of Statin Induced Myopathy [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/frequency-of-checking-creatine-kinase-in-patients-on-statins-with-elevated-transaminase-for-early-detection-of-statin-induced-myopathy/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/frequency-of-checking-creatine-kinase-in-patients-on-statins-with-elevated-transaminase-for-early-detection-of-statin-induced-myopathy/