Session Information
Date: Monday, November 8, 2021
Title: Systemic Sclerosis & Related Disorders – Clinical Poster II (1364–1390)
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Impaired exercise capacity contributes to functional impairment, negatively impacting individuals’ quality of life. Functional impairment is notable from early in the disease course of systemic sclerosis (SSc).1 Routine investigations such as pulmonary function tests (PFT) and echocardiography (TTE) often fail to adequately account for the symptom burden reported by patients.2Cardiopulmonary exercise testing (CPET) is the gold standard test for aerobic capacity. We sought to quantify the degree of exercise impairment in SSc using CPET and correlate disease manifestations, cardiac and pulmonary function and skeletal muscle abnormalities to peak VO2. Our aim was to understand the disease specific features that contribute to impaired aerobic fitness in SSc.
Methods: Thirty four patients who all fulfilled 2013 ACR/EULAR criteria for SSc were recruited. Participants underwent PFT, TTE, cardiac MRI with mapping sequences, skeletal muscle MRI and CPET. No participant had a history of myocarditis, pulmonary arterial hypertension, ischaemic heart disease, valvular heart disease or renal impairment. Using logistic and linear regression analysis we analysed the SSc manifestations and imaging features associated with peak VO2.
Results: Baseline characteristics of patients are listed in Table 1. We detected significant exercise impairment; mean % predicted peak VO2 70.18 ± 18.98%. Diffuse myocardial fibrosis was a near universal finding with 30/31 patients having elevated native T1 times, including in those patients with early limited disease and no known SSc internal organ involvement. Nine (30%) patients had areas of late gadolinium enhancement. There was evidence of diffuse myocardial oedema, with elevated T2 mapping times recorded. Skeletal muscle oedema was highly prevalent; 12 (37.50%) of participants had T2 hyperintensity on MRI. Skeletal muscle T2 hyperintensity was not associated with creatine kinase (p=0.94), ESR (p=0.79) or CRP (p=0.56).
Conclusion: Patients with SSc commonly have profoundly limited exercise capacity. This impairment is multi-factorial; subclinical cardiac and skeletal muscle involvement and impaired lung function are significantly associated with reduced peak VO2 in SSc. So-called subclinical organ involvement has negative physiological sequelae and contribute to global functional impairment. Future work is required to establish whether aerobic capacity in SSc can be improved by treatment of specific disease features or with exercise therapy.
1. Steen VD, Medsger TA, Jr. The value of the Health Assessment Questionnaire and special patient-generated scales to demonstrate change in systemic sclerosis patients over time. Arthritis & Rheumatism 1997;40:1984
2. Baron M, Sutton E, Hudson M, et al. The relationship of dyspnoea to function and quality of life in systemic sclerosis. Ann Rheum Dis 2008;67:644
 Table 1: Baseline demographics n=33
Table 1: Baseline demographics n=33
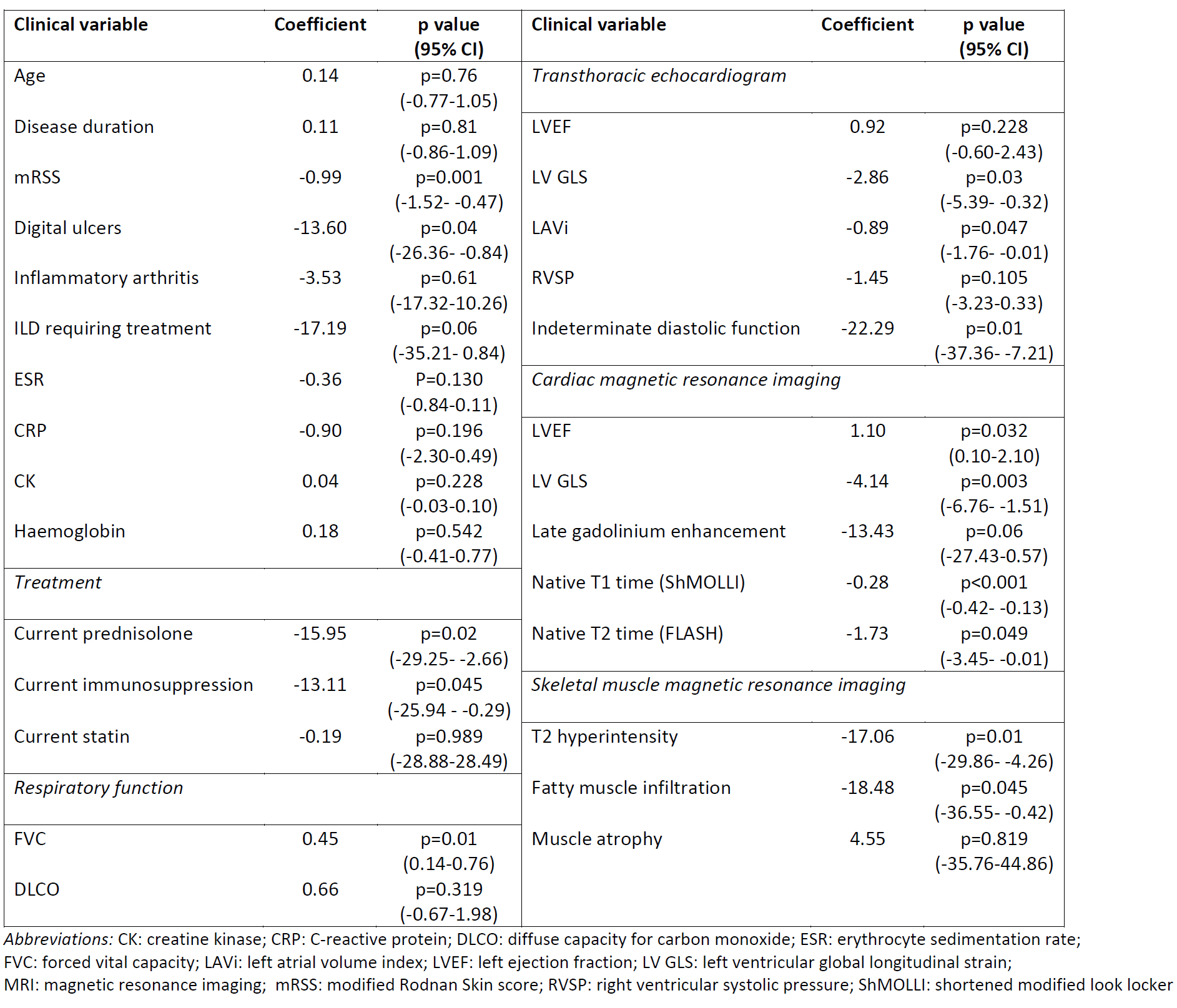 Table 2: Regression analysis of clinical characteristics associated with peak oxygen consumption (% predicted)
Table 2: Regression analysis of clinical characteristics associated with peak oxygen consumption (% predicted)
To cite this abstract in AMA style:
Ross L, Costello B, Hansen D, Lindqvist A, Brown Z, Burns A, Prior D, Stevens W, Pianta M, Perera W, La Gerche A, Nikpour M. Characterising Exercise Capacity in Systemic Sclerosis Using Cardiac Magnetic Resonance Imaging, Skeletal Muscle Imaging and Cardiopulmonary Exercise Testing [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/characterising-exercise-capacity-in-systemic-sclerosis-using-cardiac-magnetic-resonance-imaging-skeletal-muscle-imaging-and-cardiopulmonary-exercise-testing/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterising-exercise-capacity-in-systemic-sclerosis-using-cardiac-magnetic-resonance-imaging-skeletal-muscle-imaging-and-cardiopulmonary-exercise-testing/