Session Information
Date: Sunday, November 8, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster III: Cardiopulmonary Aspects
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Large, multicenter studies established the strong prognostic value of coronary artery calcium (CAC) scoring in asymptomatic individuals. Increasing CAC score is an independent predictor of worsening cardiovascular disease event risk in general patients. The prognostic significance of higher CAC score strata in the long-term cardiovascular risk in rheumatoid arthritis (RA) is unknown. We sought to evaluate the long-term cardiovascular event risk across CAC strata in a prospective, single center cohort of established RA patients without symptoms or prior diagnosis of cardiovascular disease
Methods: One hundred-fifty patients underwent computed tomography angiography for coronary atherosclerosis evaluation. CAC score was measured according to Agatston. Cardiovascular disease (CVD) events were prospectively recorded, including cardiac death, myocardial infarction, unstable angina, revascularization, stroke, claudication, and heart failure hospitalization over 6.0±2.4 years of follow-up. Unadjusted, robust Cox proportional hazards regression models evaluated CVD event risk across higher CAC strata (CAC = 1-99, CAC = 100-399 and CAC ≥ 400) compared to CAC = 0. Additional multivariable robust Cox regression models with time-varying covariates evaluated the impact of log transformed CAC or different CAC thresholds (CAC > 0 vs. CAC = 0, CAC ≥ 100 vs. CAC < 100 and CAC ≥ 400 vs. CAC < 400) on future CVD events. Models were controlled for Framingham-D'Agostino clinical risk score, time-varying current bDMARD use and time-varying CRP.
Results: Sixteen patients incurred 19 events, for a total of 2.1 (95% CI 1.3-3.3) events/100 patient-years. Increasing risk for cardiovascular events was observed across ascending CAC strata; HR 3.87 (95%CI 1.03-14.48), 6.31 (95%CI 1.38-28.91) and 16.98 (95%CI 4.50-64.10) for CAC = 1-99, CAC = 100-399 and CAC ≥ 400 respectively compared to CAC = 0 (figure 1). In fully adjusted models, CAC score associated with future event risk independently of Framingham D’Agostino score, time-varying bDMARD use and time-varying CRP (HR 1.31 [95%CI 1.04-1.66]). CAC thresholds ≥ 100 (vs. < 100) and CAC ≥ 400 (vs. < 400) in fully adjusted models similarly constituted independent predictors of long-term cardiovascular events (Figure 2).
Conclusion: Increasing CAC scores are strong, independent predictors of long-term cardiovascular events in RA patients without symptoms or prior diagnosis of cardiovascular disease.
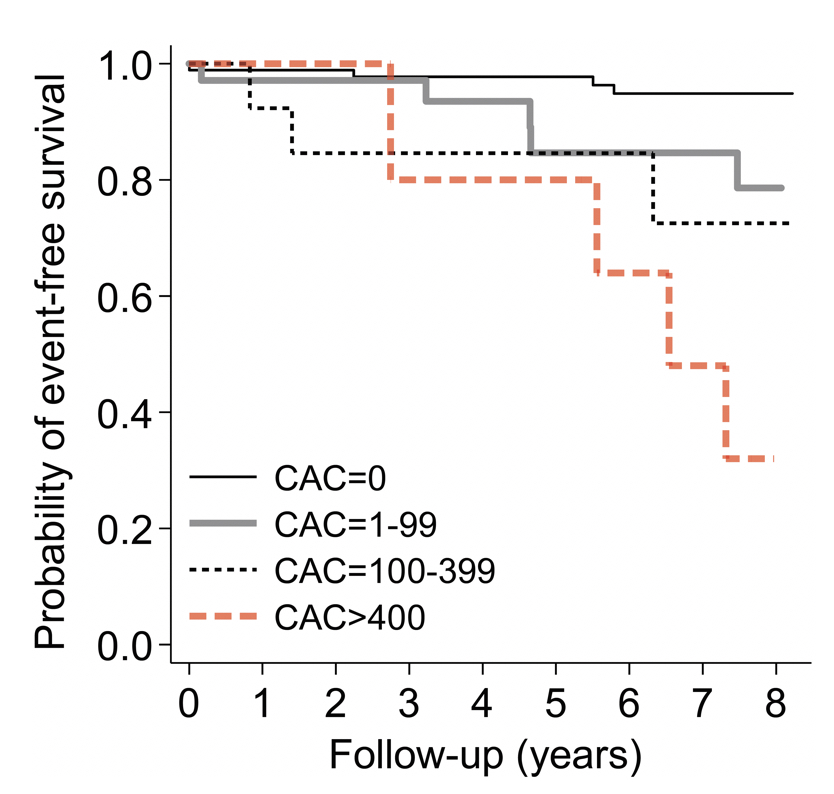 Figure 1. Increasing CAC scores associated with higher cardiovascular event risk in RA
Figure 1. Increasing CAC scores associated with higher cardiovascular event risk in RA
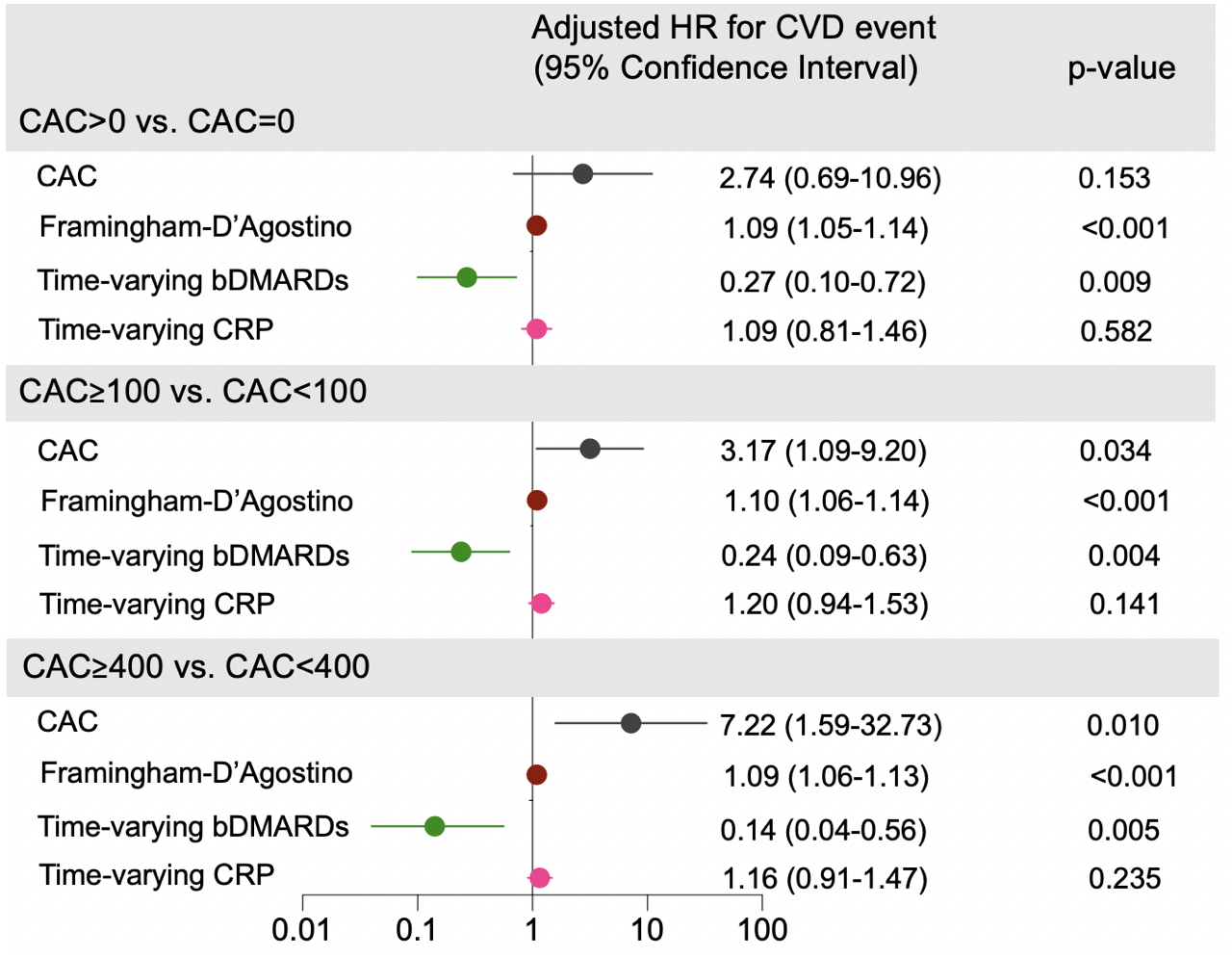 Figure 2. Impact of different CAC thresholds on cardiovascular event risk in RA
Figure 2. Impact of different CAC thresholds on cardiovascular event risk in RA
To cite this abstract in AMA style:
Karpouzas G, Ormseth S, Hernandez E, Budoff M. Subclinical Coronary Calcification Associated with Long-term Cardiovascular Outcomes in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/subclinical-coronary-calcification-associated-with-long-term-cardiovascular-outcomes-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/subclinical-coronary-calcification-associated-with-long-term-cardiovascular-outcomes-in-rheumatoid-arthritis/