Session Information
Date: Sunday, November 8, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster III: Cardiopulmonary Aspects
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: The 400 meter timed walk test has been studied as a simple summary measure of fitness that is predictive of mobility limitation and incident cardiovascular disease (CVD) events in older individuals. However, it has not been studied in the context of CVD in RA, a disease associated with physical disability, a heightened risk of atherosclerosis and myocardial dysfunction.
Methods: RA participants in a study of subclinical CVD underwent cardiac computed tomography (CT) for assessment of coronary artery calcification (CAC), 18-flourodeoxyglucose (FDG) positron emission tomography (PET) CT for assessment of aortic FDG uptake (a measure of atherosclerotic plaque inflammation) and myocardial FDG uptake (a measure of myocarditis), stressed N-13 ammonia PET for assessment of coronary microvascular dysfunction (CMD) and 3D echocardiography for assessment of left ventricular structure and function. Patients also underwent the 400m timed walk test. Generalized linear models were used to model walking endurance (i.e. total walking time) and walking speed with CVD outcomes, adjusting for potential confounders. We explored whether self-reported disability—as captured by the Health Assessment Questionnaire (HAQ)—recreated the same associations as the walk test.
Results: A total of 119 RA patients were studied [mean age=54 ± 13 years; 82% female; 74% seropositive for RF or anti-CCP; median RA duration=7 years; median DAS28-CRP=3.9]. Among these, 103 (87%) completed the walk test. Nine (8%) started but could not complete the walk, and 7 (6%) did not initiate the test. Among completers, those in the slowest time tertile were significantly older, had higher BMIs and more traditional CVD risk factors. RA duration, DAS28-CRP, tender joint count, CRP and HAQ scores were significantly higher in the slower tertile compared with the faster, but DMARD treatment did not differ. Slower completion time was associated with significantly higher CAC, aortic FDG uptake, left ventricular mass index and echocardiographic measures consistent with diastolic dysfunction (i.e. higher E/e’ ratio) (Figure). Although ejection fraction did not differ according to walk time, global longitudinal strain was worst in the slower group (Figure). Neither walk time nor walk speed was associated with myocardial FDG uptake or CMD. Modeling HAQ for walk time and walk speed did not recreate the associations. However, modeling potential confounders eliminated the associations of walk time and walk speed with all of the CVD outcomes except walk time with aortic FDG uptake, which remained significantly associated with slower walk time after adjustment for relevant confounders.
Conclusion: Although not independently associated with all CVD outcomes, walking endurance and speed is a potential summary measure of CVD risk that is a composite of multiple traditional and inflammatory risk factors for atherosclerosis and myocardial dysfunction in RA.
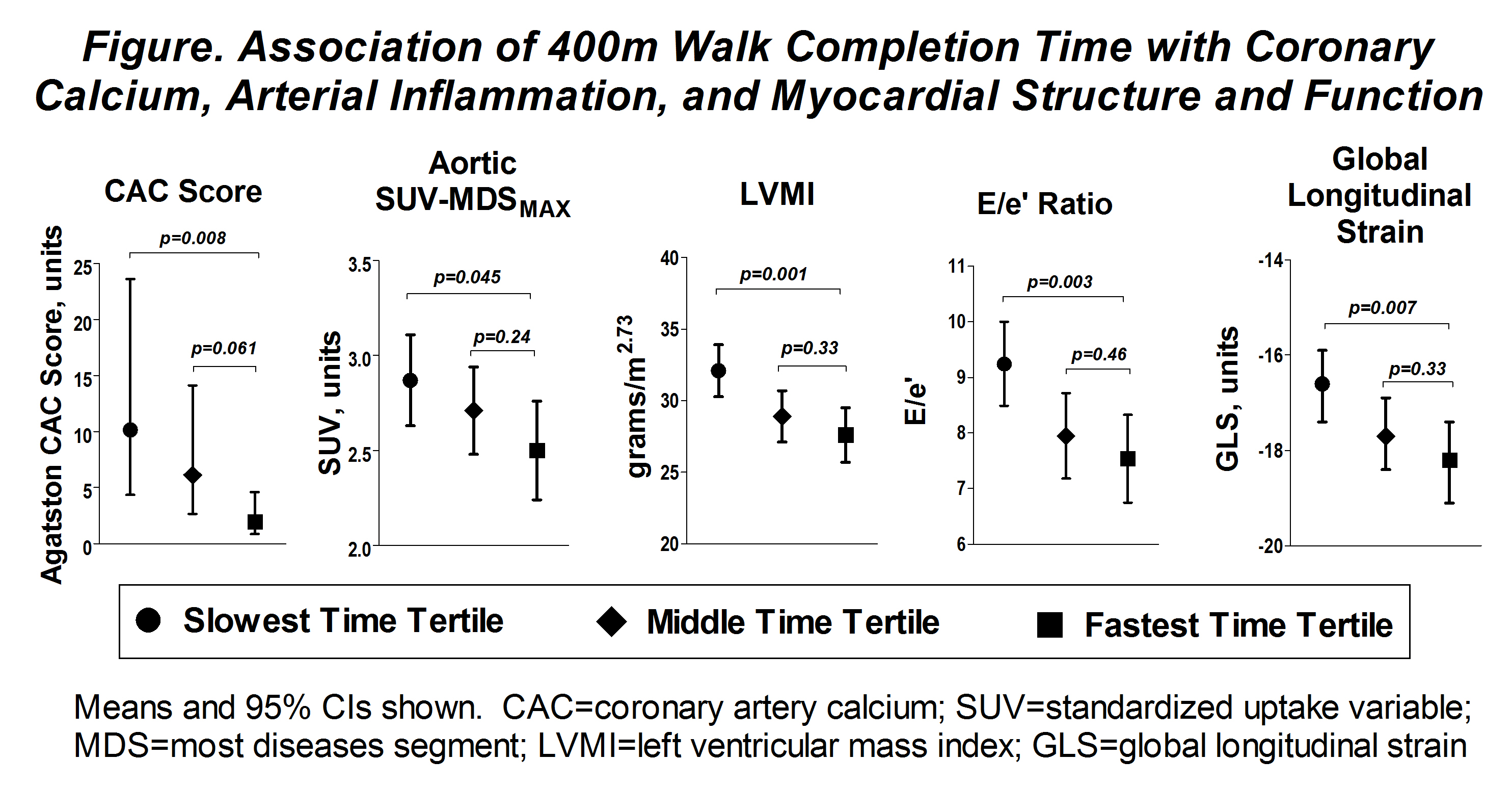 Association of 400m Walk Completion Time with Coronary Calcium, Arterial Inflammation, and Myocardial Structure and Function
Association of 400m Walk Completion Time with Coronary Calcium, Arterial Inflammation, and Myocardial Structure and Function
To cite this abstract in AMA style:
Braverman G, Bokhari S, Ito K, Bathon J, Giles J. Associations of Walking Endurance and Speed with Multiple Measures of Subclinical Cardiovascular Disease in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/associations-of-walking-endurance-and-speed-with-multiple-measures-of-subclinical-cardiovascular-disease-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/associations-of-walking-endurance-and-speed-with-multiple-measures-of-subclinical-cardiovascular-disease-in-rheumatoid-arthritis/