Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Myositis specific and associated autoantibodies are now being used more frequently in the diagnosis of idiopathic inflammatory myositis. However there is a no study looking at the utility of antibody testing in subjects presenting with HyperCKemia during routine clinical practice. We aimed to determine the usefulness of antibody testing in subjects with both symptomatic and asymptomatic hyperCKemia referred to a university affiliated practice.
Methods: This was a retrospective chart review of electronic health records of subjects in whom antibody testing was performed between January 2013 till December 2018. The autoantibody testing were performed using myomarker panel 3® (Anti-Jo-1 Ab, Anti-Mi-2 Ab, Anti-PL-12 Ab, Anti-PL-7 Ab, Anti-EJ Ab, Anti-OJ Ab, Anti-SRP Ab, Anti-Ku Ab, Anti-U2 RNP, Anti-PM/Scl-100 Ab, Anti-MDA5 Ab, Anti-NXP2 Ab, Anti-TIF-1γ Ab, Anti-SSA 52 kD IgG Ab, Anti-U1 RNP Ab, Anti-Fibrillarin U3 RNP Ab), [RDL Reference Laboratory, Los Angeles, CA], Anti-cN-1A (NT5c1A)and Anti-HMGCR Ab IgG . Baseline demographics, reason for referral, presenting symptoms, muscle enzymes (CPK, Aldolase, ALT, AST), autoantibody results, electromyography and nerve conduction studies (EMG & NCS), muscle biopsies and final clinical diagnosis were extracted from the records.
Only HyperCKemia with and without symptoms were considered for the study. We used Stat view version 5.01 (SAS Institute Inc. Cary, NC) for analysis
Results: There were 138 subjects for whom antibody testing were performed. 47 subjects met our inclusion criteria. 9 subjects were excluded from final analysis as their final diagnosis was not classified. 38 subjects included in final analysis. Baseline demographics, presenting symptoms and muscle enzyme levels are presented in table 1. Results of EMG & NCS, myositis antibody and final clinical diagnosis details are presented in table 2. The relationship between CPK, final diagnosis and myositis antibodies are shown in Figure 1. Subjects with moderate elevation of CPK and positive antibody are more likely to have polymyositis. Subjects with mild elevation of CPK and positive antibody are more likely to have inclusion body myositis. Negative antibody subjects are more likely to be diagnosed with idiopathic hyperCKemia and metabolic myopathy.
Antibody positive was statistically associated with polymyositis, inclusion body myositis with a chi square of 25.94 with p value 0.002 with 9 degree of freedom.
Antibody positivity was statistically associated with inflammatory myositis on muscle biopsy with a chi square of 16.37 p value 0.01 with 6 degree of freedom.
Metabolic myopathy will likely have negative myositis antibody test.
Conclusion: Subjects presenting with asymptomatic or symptomatic hyperCKemia and having positive antibody, are more likely to have positive muscle biopsy and final diagnosis of inflammatory myositis. Therefore, performing initial antibody testing in such cases would help clinicians in pursuing these cases with EMG & muscle biopsy.
 Table 1. Baseline Characteristics of study population(N = 47)
Table 1. Baseline Characteristics of study population(N = 47)
 Table 2. Muscle biopsy, EMG & NCS, Myositis antibody and Final clinical diagnosis
Table 2. Muscle biopsy, EMG & NCS, Myositis antibody and Final clinical diagnosis
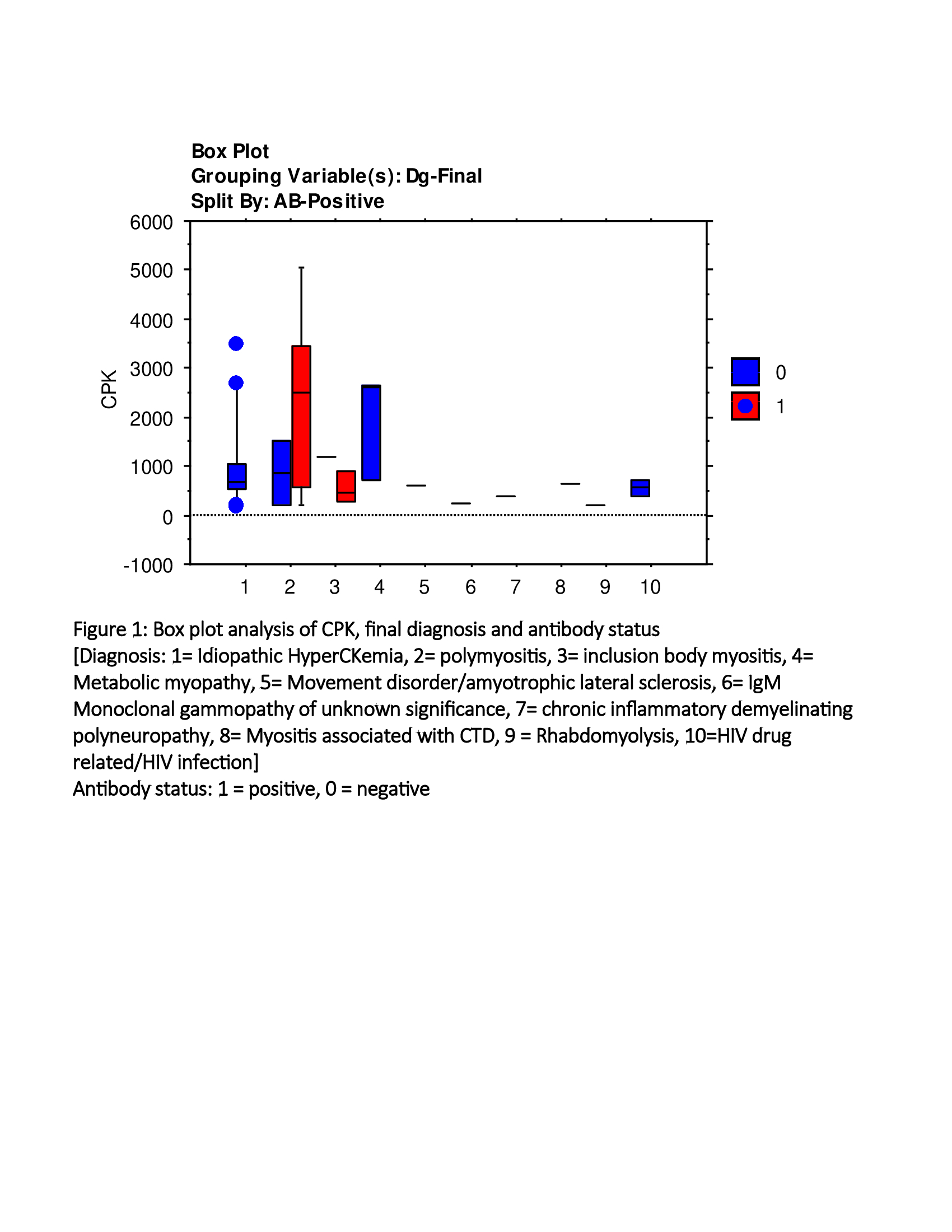 Figure 1: Box plot analysis of CPK, final diagnosis and antibody status
Figure 1: Box plot analysis of CPK, final diagnosis and antibody status
To cite this abstract in AMA style:
Gupta S, Pattanaik D, Bertorini T, Afreire A. Diagnostic Utility of Myositis Antibodies in HyperCKemia: A University Affiliated Single Center Retrospective Study [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/diagnostic-utility-of-myositis-antibodies-in-hyperckemia-a-university-affiliated-single-center-retrospective-study/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-utility-of-myositis-antibodies-in-hyperckemia-a-university-affiliated-single-center-retrospective-study/