Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Until the COVID 19 crisis we initiated DMARD(s) and Biologic therapies using shared medical clinics. More than 30 patients could seen per week, with a maximum of 6 per group, for each different medication to be started, (see fig 1). This allowed us to manage the increase in workload, and start patients efficiently on their medications, both safely, and within 10 working days. This took 3-4 hours per week of Rheumatology nurse time.
However, with the onset of the pandemic, we had to stop these clinics immediately, but, we did not have capacity to start everyone on their medications in a timely manner by telephone. Telephoning each individual took > 9 hours per week.
Methods: We scripted and organised the filming of 10 short healthcare videos very rapidly (www.torbayandsouthdevon.nhs.uk), to give patients all the information they required to start a range of DMARDs and biologics.
We developed a new algorithm (Fig 2) and now patients are asked to view the relevant video, contact our department to confirm they understand the safety monitoring, risks, potential side effects, dose increases etc. As soon as they confirm by email they are happy to start treatment, a prescription is generated and emailed to the hospital outpatient pharmacy, where it is dispensed and delivered to the patient’s home (usually within 3 working days). We also send them a follow up reminder letter about blood test monitoring etc (with copy to their GP) and a ‘shared care agreement’ to their GP. Alternatively, if they are uncertain about anything, we organise for them to have a telephone clinic appointment with a specialist nurse.
Results: Of those requiring DMARDs, 55% reviewed the video, completed the checklist and confirmed by email they were happy to start treatment, within 24-hours. A further 26% completed the process within 3 days.
Almost half the patients (48%) were starting DMARDs for the first time, of those 8% requested a telephone consultation to discuss treatment further with the Rheumatology nurses. None of the patients already taking a DMARD and due to start a second medication required a telephone clinic appointment.
As this is a new service, we asked for feedback, receiving replies from 26%, all scoring between 9/10 and 10/10.
Conclusion: This has altered the way we work and we will continue with this approach over the long term. It has reduced the necessity for face-to-face appointments, enabled us to start patients on their rheumatology medications more quickly and efficiently than previously, allowed the nursing staff time to spend more time working in our telephone clinic and we have had excellent feedback. Although, we are aware, this is at a cost of no peer-to-peer interaction, which has been of value in the past.
 Fig 1: Our original Shared Medical Appointment Approach to start DMARDs and Biologics
Fig 1: Our original Shared Medical Appointment Approach to start DMARDs and Biologics
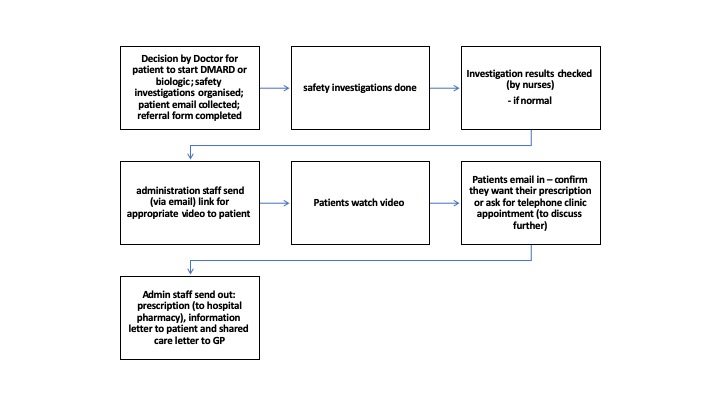 Fig 2: Our digital solution for medication clinics
Fig 2: Our digital solution for medication clinics
To cite this abstract in AMA style:
Penford R, Reith A, Wren E, Mackay K. Going Digital Due to COVID 19 Crisis: A Rapid Reorganisation of Medication Clinics [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/going-digital-due-to-covid-19-crisis-a-rapid-reorganisation-of-medication-clinics/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/going-digital-due-to-covid-19-crisis-a-rapid-reorganisation-of-medication-clinics/