Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with diffuse cutaneous systemic sclerosis (dcSSc) are at greater risk of developing interstitial lung disease (ILD) than patients with limited cutaneous systemic sclerosis (lcSSc). In the SENSCIS trial in patients with SSc-ILD, nintedanib reduced the rate of decline in forced vital capacity (FVC) vs placebo over 52 weeks, with no difference between groups in the change from baseline in modified Rodnan skin score (mRSS). We analyzed data from the SENSCIS trial in subgroups of patients with lcSSc or dcSSc.
Methods: Patients with SSc-ILD with onset of first non-Raynaud symptom < 7 years before screening and ≥10% fibrosis of the lungs on a high-resolution computed tomography (HRCT) scan were randomized to receive nintedanib 150 mg bid or placebo. We analyzed outcomes and adverse events over 52 weeks in subgroups of patients with lcSSc or dcSSc at baseline.
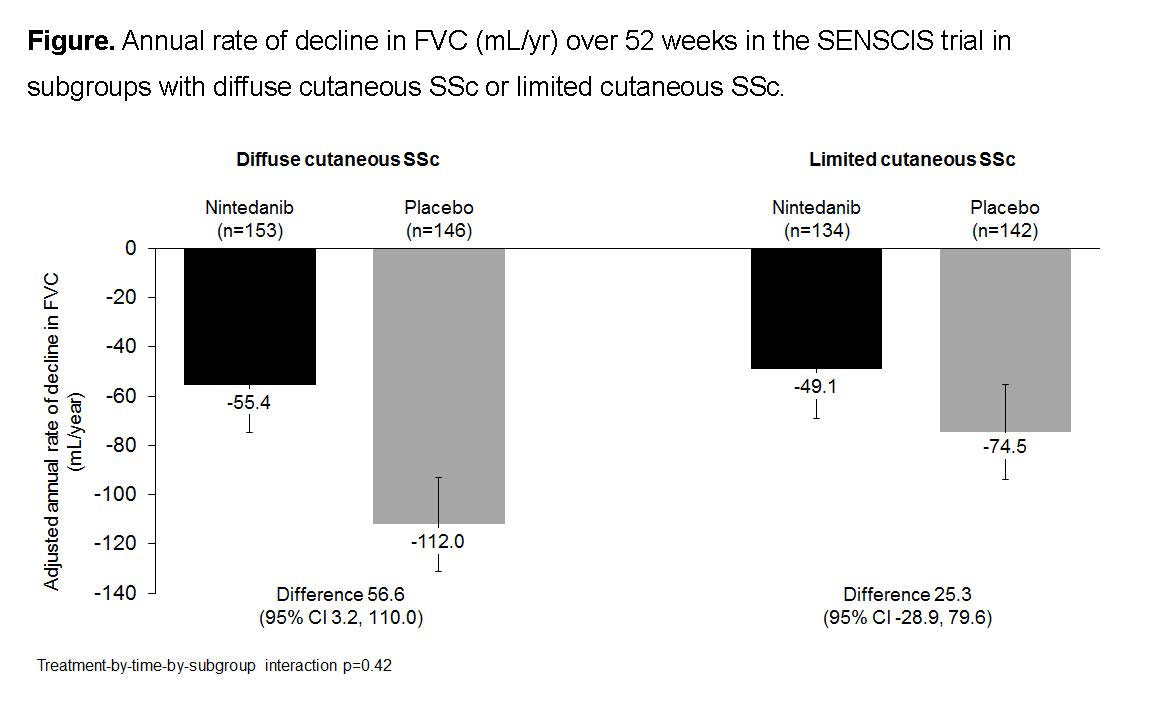
Results: Of 288 patients treated in each group, 153 (53.1%) and 146 (50.7%) in the nintedanib and placebo groups, respectively, had dcSSc. At baseline, in patients with dcSSc and lcSSc, respectively, mean (SD) FVC (mL) was 2461 (797) and 2542 (755), FVC % predicted was 70.5 (16.3) and 74.8 (16.8), and modified Rodnan skin score (mRSS) was 16.7 (8.8) and 5.2 (4.1). In the placebo group, the annual rate of FVC decline was numerically greater in patients with dcSSc than lcSSc (-112.0 vs -74.5 mL/year). Nintedanib reduced the rate of FVC decline both in patients with lcSSc and dcSSc. The treatment effect of nintedanib on FVC decline was numerically greater in patients with dcSSc than lcSSc, but no difference in the treatment effect between subgroups was detected (treatment-by-time-by-subgroup interaction p=0.42) (Figure). In the nintedanib and placebo groups, respectively, absolute declines in FVC >5% predicted at week 52 were seen in 22.2% and 28.8% of patients with dcSSc (OR 0.71 [95% CI 0.42, 1.20]) and 18.7% and 28.2% with lcSSc (OR 0.59 [0.33, 1.04]) (treatment-by-subgroup interaction p >0.05). Adjusted mean absolute changes from baseline in mRSS at week 52 in the nintedanib and placebo groups were -1.6 and -1.5 in patients with dcSSc (difference -0.2 [95% CI -1.2, 0.8]) and -2.7 and -2.5 in patients with lcSSc (difference -0.3 [-1.3, 0.8]; treatment-by-subgroup interaction p >0.05). The adverse event profile of nintedanib was similar between patients with dcSSc and lcSSc.
Conclusion: In the SENSCIS trial in patients with SSc-ILD, the rate of decline in FVC in patients who received placebo was greater in patients with dcSSc than lcSSc. Nintedanib reduced the rate of FVC decline both in patients with dcSSc and lcSSc. The treatment effect of nintedanib was numerically greater in patients with dcSSc than lcSSc, but statistical testing did not indicate heterogeneity in the treatment effect between the subgroups. No effect of nintedanib was demonstrated on skin fibrosis assessed using the mRSS.
To cite this abstract in AMA style:
Kuwana M, Highland K, Gahlemann M, Denton C, Fischer A, Mayes M, Steen V, Khanna D, Allanore Y, Girard M, Alves M, Stowasser S, Distler O. Effects of Nintedanib in Patients with Diffuse and Limited Cutaneous Systemic Sclerosis and Interstitial Lung Disease: Subgroup Analysis of the SENSCIS Trial [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/effects-of-nintedanib-in-patients-with-diffuse-and-limited-cutaneous-systemic-sclerosis-and-interstitial-lung-disease-subgroup-analysis-of-the-senscis-trial/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effects-of-nintedanib-in-patients-with-diffuse-and-limited-cutaneous-systemic-sclerosis-and-interstitial-lung-disease-subgroup-analysis-of-the-senscis-trial/