Session Information
Date: Tuesday, November 10, 2015
Title: Osteoarthritis - Clinical Aspects Poster II: Biomarkers, Biomechanics and Health Services Research
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Development of disease modifying
medication for osteoarthritis (OA) is desirable, but the target tissue of such
treatment remains unclear. We have previously shown that proliferative and
hyperemic synovial tissue is rare in joints affected by erosive osteoarthritis
(EOA), if power Doppler ultrasound (US) is used as the detecting instrument.
Doppler ultrasound gives indirect information about blood flow by assessing
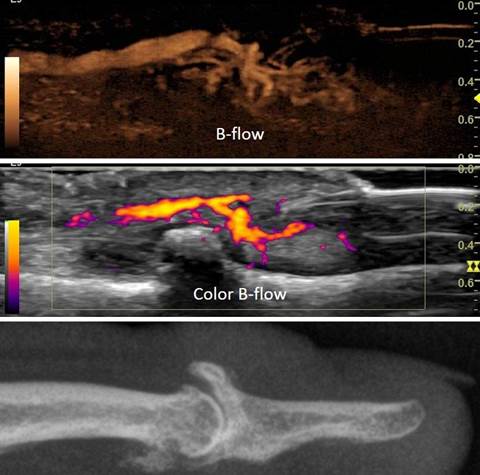
amplitude or velocity of a frequency shift. In contrast, B-flow ultrasound
directly visualizes blood flow, and can visualize synovial hyperemia in a
precise (flow only in the vascular lumen) and sensitive (small vessels)
fashion. No previous studies have used B-flow ultrasound to assess synovial
hyperemia.
The aim of this study was to assess synovial proliferation
and synovial hyperemia in proximal interphalangeal and distal interphalangeal joints
of patients with a radiologic diagnosis of OA or EOA using high-frequency
B-mode gray scale US and B-flow US.
Methods: Joints affected by OA or EOA based on bilateral
hand radiographs in 3 planes were then examined sonographically. For
enrollment, the assessment of the MSK radiologist was counted. Gray scale US,
native B-flow US and color B-flow still images and 3-second video clips were
obtained by a rheumatologist with 20 years of experience in MSK US, certified
in rheumatologic US (RT). All US and B-flow scans were performed on a GE Logiq
E9 built 2014 machine, with an 18 MHz small footprint probe using a B-flow
software package. Vascular factory settings were optimized for low flow in
fingers. Distension of the hyperechoic, fibrous joint capsule was scored for GS
synovitis from 0-3 (absent, mild, moderate, severe), analogous to scoring for
RA. Intra-articular synovial blood flow was scored from 0-3 (no flow,
individual signals, involving less, and equal to/ more than half the area of
detected synovitis). Total scores for EOA patients were compared with OA
patients.
Results: 559 still images and video clips were obtained. 84
joints of 20 consecutive OA and EOA patients were examined: DIP n=55; IP/PIP
n=29. EOA patients, n=11 (55%); OA, n=9, (45%) as determined prior to US by the
reading radiologist. Age range was 51-88 years; mean age 68. Female, n=16;
male, n=4.
Resulting scores: Gray scale (score=n) 0=45; 1=31; 2=4; 3=2.
B-flow (score=n) 0=81; 1=4; 2=1; 3=0. Mean GS score EOA=56.6; OA=53. Scores for
intra-articular B-flow were too low to compare.
Conclusion: B-flow US was well suited to detect blood flow
in small digital vessels. While physiologic flow in soft tissues adjacent to
joints was seen in all images and video clips, intra-articular, synovial blood
flow was rarely observed in OA or EOA patients. Synovial proliferation, if
present, was mild and appeared to be due to mechanical distension of the joint
capsule by osteophytes. No significant difference in mean GS synovitis score
was observed between OA and EOA patients.
To cite this abstract in AMA style:
Thiele RG, Anandarajah AP, Ritchlin CT. B-Flow Imaging of Synovial Tissue in Osteoarthritis [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/b-flow-imaging-of-synovial-tissue-in-osteoarthritis/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/b-flow-imaging-of-synovial-tissue-in-osteoarthritis/