Session Information
Date: Sunday, November 13, 2016
Title: Rheumatoid Arthritis – Clinical Aspects - Poster I: Clinical Characteristics/Presentation/Prognosis
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Erosive damage to small joints is a hallmark feature of rheumatoid arthritis (RA). The degree to which early erosive damage contributes to joint pain in well-controlled disease is incompletely understood. The use of magnetic resonance imaging (MRI) combined with erosion segmentation software, such as Early Erosions in Rheumatoid Arthritis (EERA), provides opportunity for the study of small, early erosions. Our objective was to apply multiple linear regression modeling to determine how low levels of erosive damage contribute to joint pain in RA.
Methods: From a single rheumatology clinic, 125 patients satisfying early RA referral criteria were included. Clinical and laboratory disease measures were captured. MRI of both hands were acquired, and a single reader used EERA software to compute total erosive damage in the metacarpophalangeal (MCP) joints, in mm3. A multiple linear regression model was constructed, with the dependent variable as patient-reported finger joint pain, rated none, mild, moderate, or severe. Predictor variables included age, sex, symptom duration > 1 year, disease-modifying antirheumatic drug (DMARD) or biologic use over preceding 3 months, disease activity score using erythrocyte sedimentation rate (DAS28 ESR), and MCP joint erosion volume. Sensitivity analyses were conducted, using daily or weekly history of illness-associated pain, rated on visual analog scale (VAS, 0 to 100), as alternative dependent variables.
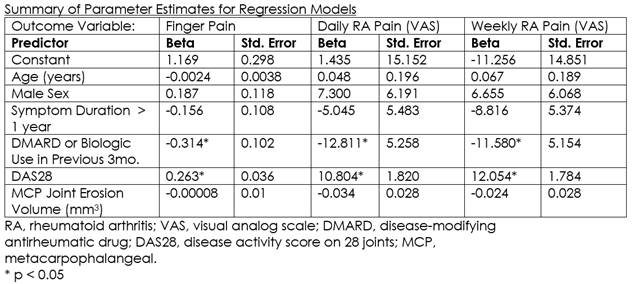
Results: Patients were 76% female, 81% Caucasian, mean (SD) age 56 (13) years, symptom duration 4.3 (5.0) years, DAS28 ESR 4.5 (1.4), pain VAS 45 (31), with 55% using DMARD or biologic over the preceding 3 months. Mean MCP erosive damage was low at 37 (91) mm3. The regression model (R2 = 0.225, p < 0.001) showed no statistically significant relationship between finger pain and erosion volume (B = 0.00008, p = 0.896). Among other predictor variables, only DAS28 ESR (B = 0.263, p < 0.001) and 3 month history of DMARD or biologic use (B = -0.314, p = 0.002) were significantly associated with finger pain. Regression estimates were similar when right and left hands were analyzed independently. Using either of weekly or daily patient-reported illness-associated pain VAS as the dependent variable, again only DAS28 ESR and 3 month history of DMARD or biologic use were significant model predictors.
Conclusion: Low level of MCP joint erosive damage was not associated with increased finger pain or illness-associated pain in well-controlled RA. Lower acute disease activity and concurrent DMARD or biologic therapy were associated with decreased pain. Longitudinal models may help identify the threshold at which MCP joint damage becomes an important contributor to finger pain.
To cite this abstract in AMA style:
Jessome MA, Beattie KA, Bensen WG, Bobba RS, Cividino A, Emond PD, Gordon C, Hart L, Ioannidis G, Larche M, Lau A, Tavares R, Tytus S, Adachi JD. What Is the Relationship Between Early Metacarpophalangeal Erosions on MRI and Joint Pain in Rheumatoid Arthritis? [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/what-is-the-relationship-between-early-metacarpophalangeal-erosions-on-mri-and-joint-pain-in-rheumatoid-arthritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/what-is-the-relationship-between-early-metacarpophalangeal-erosions-on-mri-and-joint-pain-in-rheumatoid-arthritis/