Session Information
Date: Tuesday, October 23, 2018
Title: Metabolic and Crystal Arthropathies – Basic and Clinical Science Poster II
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: To improve quality of care for patients with gout, two hospitals in the Netherlands initiated a protocolized gout clinic. One clinic adopted a patient-centred (PC-) strategy – emphasizing a shared decision based on serum uric acid (sUA) and patient satisfaction with gout control – and the other clinic adopted a strict sUA (≤0.30 mmol/L) target (UA-) strategy, with early combination of xanthine oxidation inhibitors (allopurinol) with uricosurics if the target was not reached and fractional uric acid excretion was below 4% (two modes of action (2MoA)).
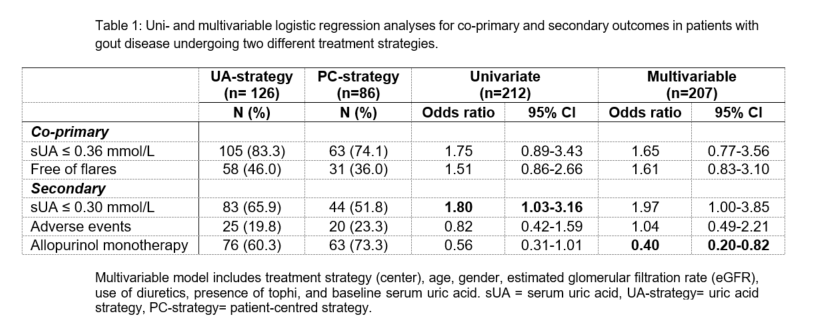
Methods: Patients newly diagnosed with gout by the rheumatologist and having a follow-up between 9-15 months after the first visit were included. Co-primary outcomes were the proportion of patients reaching a sUA ≤0.36 mmol/L, and the proportion of patients free of flares. Secondary outcomes were the proportion of patients with a sUA ≤0.30 mmol/L, requiring treatment intensification beyond allopurinol (and especially 2MoA), and experiencing adverse events. Independent t-tests or chi-square were used to test differences in outcomes between strategies, and logistic regressions to adjust the effect of center on outcomes for baseline confounders.
Results: In total, 255 and 142 new patients attended the UA and PC-strategy clinic, respectively, for the first time. Of the initial patients, 29/255 (11%) vs 13/142 (9%) patients stopped prematurely clinical follow-up and 6/255 (2%) vs 11/142 (8%) patients died. Finally, 126 and 86 patients had a follow-up assessment between 9-15 months after inclusion. Diagnosis of gout was further confirmed by ACR/EULAR classification criteria for 122/126 (97%) patients in the UA-strategy vs 51/86 (59%) patients in the PC-strategy (p<0.001), respectively. In the UA-strategy 105/126 (83%) patients compared to 63/86 (74%) patients in the PC-strategy (p=0.10), reached the threshold of ≤0.36 mmol/L and 58/126 (46%) vs 31/86 (36%) patients (p=0.15) were free of flares (table 1). In the UA-strategy 76/126 (60%) patients were on allopurinol monotherapy compared to 63/86 (73%) in those receiving the PC-strategy (p=0.05). 2MoA therapy was significantly more frequent in the UA-strategy (n=21 (17%) vs n=1 (1%), p<0.001), yet the number of registered adverse events was not different (n=25 (20%) vs n=20 (23%), p=0.55). After adjustment for baseline confounders, the UA-strategy had a slightly higher but non-siginifiant chance to reach sUA ≤0.36 mmol/L and to be free of flares, but required significantly more therapy intensification.
Conclusion: A strict UA-strategy resulted in a non-significant higher proportion of patients reaching the UA target (≤0.36 mmol/L) and free of flares. This was accomplished with significant more therapy intensification from allopurinol monotherapy to 2MoA therapy, without a significant difference in adverse events.
To cite this abstract in AMA style:
te Kampe R, van Durme C, Janssen M, Boonen A, Jansen T. What Can Variation in Clinical Practice Teach Us about Treatment Strategies for Patients with Gout? [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/what-can-variation-in-clinical-practice-teach-us-about-treatment-strategies-for-patients-with-gout/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/what-can-variation-in-clinical-practice-teach-us-about-treatment-strategies-for-patients-with-gout/