Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Use of telemedicine has increased substantially. Our overall goal was to assess the utility of a standardized video joint exam and infrared thermal imaging as virtual tools to determine joint status during telemedicine visits.
Methods: Adults and children aged ≥4 and with an established diagnosis of inflammatory arthritis and suspected active inflammation in at least one knee, ankle/subtalar, elbow, or wrist joint were enrolled. A joint exam performed by the in-person clinician during routine visits was recorded as the gold standard of joint status. On the same day, participants completed a clinical research visit consisting of completion/obtainment of: 1. a questionnaire, 2. thermal images of hands, wrists, elbows, knees, ankles and feet, and 3. a standardized video joint exam. A follow-up research visit was conducted along with a clinical visit ≥3 months later. All the data collected except the clinical joint exam and assessment recorded by the in-person clinician was used to simulate “virtual visits” for “virtual” physicians to review. In order to determine the added value of each component of patient-generated data, the virtual physicians recorded their impression of the 72 joint exam and physician global assessment (PGA) sequentially: 1. after viewing the results of the patient questionnaire, primary rheumatologist’s interval history, and lab results (if available), 2. after viewing the video joint exam, and 3. after viewing the thermal images and thermal imaging report. Interrater reliability statistics were calculated by cohort, joint, and review type (history only, history + video, history + video + thermal), and include both baseline and follow-up assessments. Sensitivity and specificity were calculated by joint, cohort, review type, time (baseline and follow-up) and reviewer seniority.
Results: We enrolled 100 adults and 101 children (Table 1). At every virtual assessment (history only, history + video, and history + video + thermal report), there was a significant positive correlation between in-person and virtual physicians regarding the PGA. Regarding total active joint counts, there was a significantly positive correlation between in-person and virtual physicians at every assessment, except for when the adult virtual doctors were provided with history only (Table 2). Regarding the sensitivity and specificity for detecting inflammatory arthritis in the virtual setting, sensitivity was low and generally did not improve as more information was provided (13-83% for pediatric providers, and 0-58% for adult providers). However, specificity was high at nearly every time point assessed (57-97% for pediatric providers and 52-86% for adults). Agreement between the virtual physicians generally decreased as more information was added (Figure 1).
Conclusion: Our study showed that history complemented with asynchronous video exam reviewed by rheumatologists led to moderately consistent assessment as in-person providers. Thermal imaging results did not yield additional benefit towards accurate joint assessment in the present study.
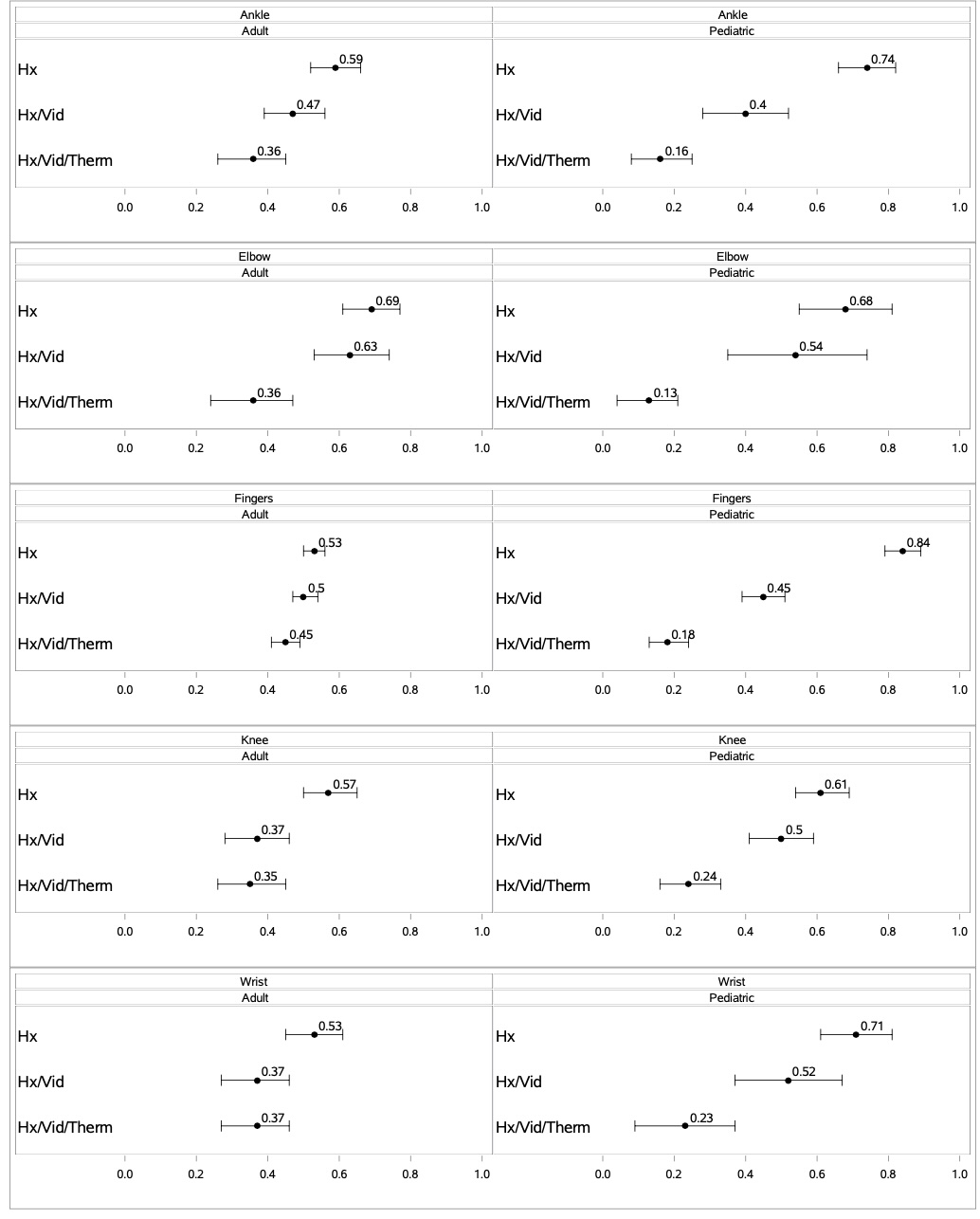 Table 1. Patient Characteristics
Table 1. Patient Characteristics
.jpg) Table 2. Correlation of PGA and Joint Count by Virtual Physicians with In-person Physician by Seniority and Review Type
Table 2. Correlation of PGA and Joint Count by Virtual Physicians with In-person Physician by Seniority and Review Type
.jpg) Figure 1. Kappa (95% CI) By Level of Information Among Adult and Pediatric Patients
Figure 1. Kappa (95% CI) By Level of Information Among Adult and Pediatric Patients
To cite this abstract in AMA style:
Thomason J, Pooni R, Sullivan E, Liau A, Van den Bogaerde S, Hamilton I, Paluvayi S, Tran M, Robles-Navarro J, Muse I, Luey A, Klein A, Biswas D, Partridge S, Lee T, Bays A, Hughes G, Ferucci E, Zhao Y. Validation of Asynchronous Telehealth Visit for Adults and Children with Inflammatory Arthritis and Feasibility of Applying Thermal Imaging during Visits [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/validation-of-asynchronous-telehealth-visit-for-adults-and-children-with-inflammatory-arthritis-and-feasibility-of-applying-thermal-imaging-during-visits/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/validation-of-asynchronous-telehealth-visit-for-adults-and-children-with-inflammatory-arthritis-and-feasibility-of-applying-thermal-imaging-during-visits/