Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: In most areas in the United States, access to rheumatologists for an initial evaluation is a major challenge resulting in long wait times for first visits. Seeking to address this problem, a new pathway was implemented utilizing rapid telehealth visits (RTV) for new patients with a low suspicion for rheumatologic disease, based on either chart review or self-reported reasons for visit. This report describes the results of this model at a large academic practice, including impact on access, revenue, and operations.
Methods: The Division of Rheumatology is a large academic medical practice with 33 faculty members and 3 advanced practice providers (APPs) seeing >30,000 patients annually across 5 sites.
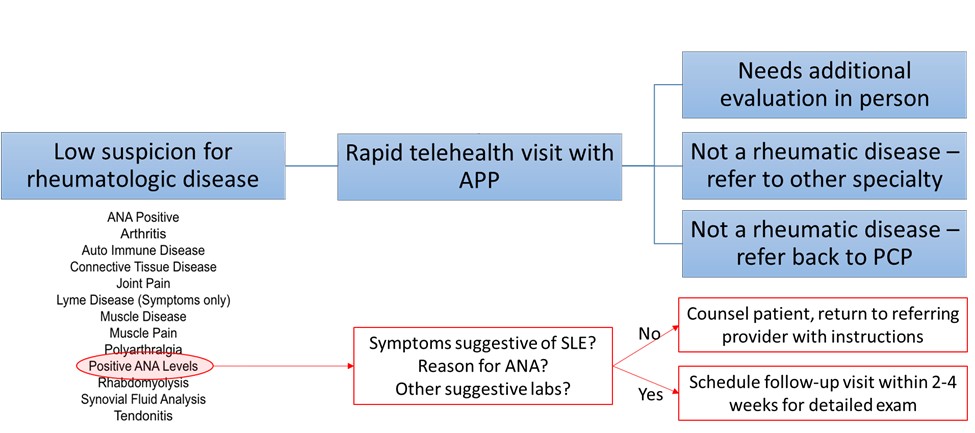
There are two pathways in which a patient could be scheduled for an RTV. Starting in February, 2021, all internal consults were reviewed by a rheumatology APP via chart review. If there was low suspicion that the patient had a rheumatologic disease, the patient was deemed eligible for an RTV. External referrals underwent a screening process implemented by our centralized access center to determine the reason for visit. If a patient reported a diagnosis that fit our pre-determined list of appropriate diagnoses, an RTV visit was offered. Diagnoses included positive antinuclear antibody, positive rheumatoid factor, non-specific joint pain, chronic pain, and other similar scenarios. Exclusion criteria included second opinions, patient’s geographic location, and reason for visit.
Twenty- or thirty-minute virtual appointments were designated for this patient population on APP telehealth schedules, rather than the usual 60-minute in-person new-patient slots. If indicated, these patients were evaluated in the office for a more comprehensive visit, including a physical exam.
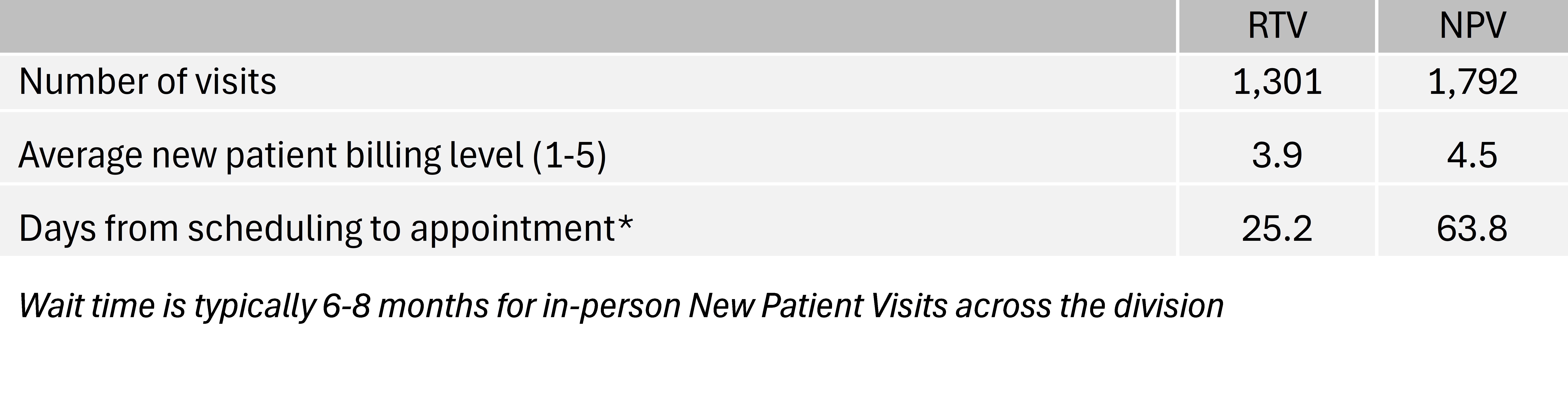
Results: Between February 2021 and May 2024, 1,301 patients completed an RTV. Average time to initial visit via RTV was 25.2 days compared to 63.8 days for those seen via an in-person new patient visit (NPV). Of those seen via RTV, 556 (42%) were then seen for at least one follow-up visit, and 253 (20%) patients required more than one follow-up visit. The average billing level for these visits was comparable to longer NPVs among the same group of APPs: 3.9 for RTV, 4.5 for NPV. However, the RTVs resulted in more RVUs per session since two to three times as many visits were completed in that same hour. There was also strong satisfaction with the program by both APPs and physicians who saw some of the patients in follow-up. Several aspects of the program continue to be addressed, including measuring visit quality, addressing panel size for APPs resulting from these visits, and determining appropriate diagnoses to include.
Conclusion: RTVs provide an accessible and rapid means of assessment for patients referred to large academic practices with low likelihood of rheumatologic disease. This model of care delivery is time- and cost-effective with strong satisfaction among patients and providers. Such a program can be part of creative strategies to address critical shortages of rheumatologists.
To cite this abstract in AMA style:
Amudala N, McCauley S, Kanoff A, Koplin J, Merkel P, Craig E. Utilization of Rapid Telehealth Visits by Advanced Practice Providers for New Patients Referred to a Large Academic Practice with Low Suspicion for Rheumatologic Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/utilization-of-rapid-telehealth-visits-by-advanced-practice-providers-for-new-patients-referred-to-a-large-academic-practice-with-low-suspicion-for-rheumatologic-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/utilization-of-rapid-telehealth-visits-by-advanced-practice-providers-for-new-patients-referred-to-a-large-academic-practice-with-low-suspicion-for-rheumatologic-disease/