Session Information
Date: Monday, October 27, 2025
Title: (1553–1591) Systemic Sclerosis & Related Disorders – Clinical Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: In 2019 a European expert consensus suggested that all patients with systemic sclerosis (SSc) should be screened with HRCT for interstitial lung disease (ILD) at diagnosis, regardless of the presence of risk factors (RF). However, in the absence of RF or suggestive symptoms or signs, the probability of finding ILD is low. Our aim was to assess rate of ILD and its severity in the absence of clinical suspicion (CS) or RF for ILD in patients with SSc at diagnosis.
Methods: Retrospective study of patients with a recent diagnosis of SSc from January 2020 to January 2025 who were under follow up in a dedicated SSc clinic in Madrid, Spain. Patients with CS and/or RF for ILD were compared with those without CF or RF. CS was defined as presence of dyspnea or crackles. RF were defined as ATA+, diffuse cutaneous involvement or active smokers. Severe ILD was defined as disease characterized either by progression observed in PFT or the requirement for immunosuppressive and/or antifibrotic treatment. Categorical variables were described as proportions and/or percentages, while continuous variables were shown as mean or median and standard deviation (SD) or interquartile range (IQR). The Student t test and X2 test were used to compare data, when appropriate.
Results: 70 patients were diagnosed of SSc during the study period, 90% were screened with HRCT at diagnosis, therefore 63 patients were analyzed. Main characteristics are reported in Table 1. There were no differences in age, sex, race, presence of ACA, time in follow up and organ involvement other than ILD between both groups. In 26 (41.3%) patients there were no CS or RF for ILD. ILD was diagnosed in 3 (11.5%) patients without RF or CS compared to 18 (45.9%) in the group with CS and/or RF (p< 0.001). After a mean of 28.4 months of follow-up, none of the patients in the group without CS or RF required treatment for ILD, compared to 10 patients (27%) and 4 patients (10.8%) in the other group who required IS and antifibrotic therapy, respectively (Table 2). Serial pulmonary function tests (PFT) were available in 15/20 (75%) patients with ILD, 2/3 patients without CS or RF had serial PFT, both without deterioration. On the contrary, 13/17 patients with CS and ILD had serial PFT, 53.8% had deterioration of PFT at baseline and 38.5% showed worsening during follow-up. There were no differences in time in follow-up PFT between groups (no CS mean 41.5 months [SD 16.3], CS: mean 32.3 months [SD 12.3], p=0.361).
Conclusion: In our cohort, in absence of CS or RF for ILD, only 11.5% had ILD and none required IS or antifibrotic therapy. Despite the presence of ILD in HRCT at diagnosis, the presence of CS or RF seems to be a key factor identifying patients requiring treatment or in risk of progression during initial follow up. It is necessary to be very cautious with the interpretation of radiological findings in patients without RF because their clinical significance is probably minimal.
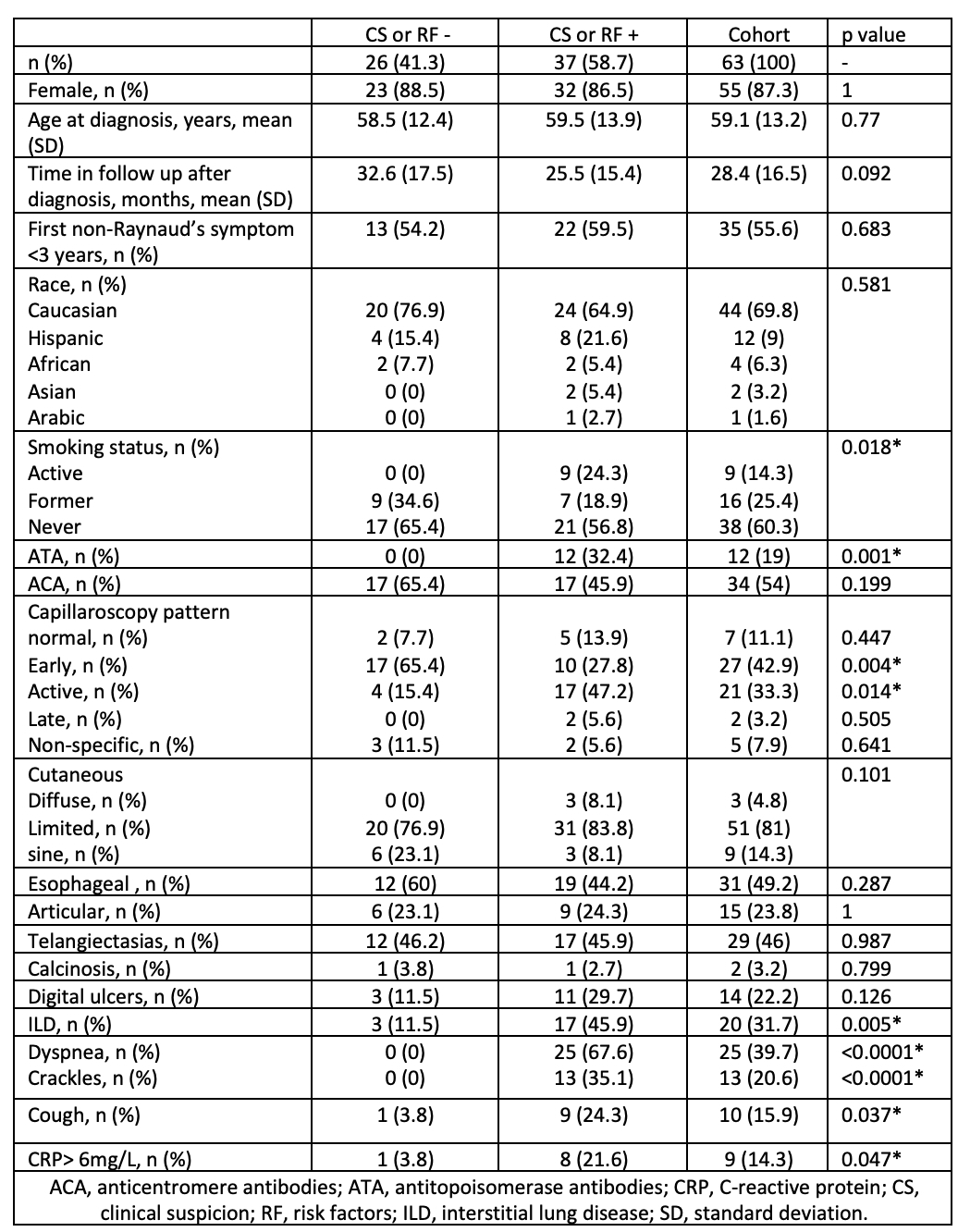 Table 1: Main clinical characteristics regarding presence of CS or RF for ILD
Table 1: Main clinical characteristics regarding presence of CS or RF for ILD
.jpg) Table 2: HRCT findings, PFT and treatment regarding presence of CS or RF
Table 2: HRCT findings, PFT and treatment regarding presence of CS or RF
To cite this abstract in AMA style:
de la Puente-Bujidos C, Garcia Fernandez A, García García V, Loarce J, Garrote-Corral S. Usefulness of HRCT in screening of interstitial lung disease in patients with systemic sclerosis without risk factors of clinical suspicion [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/usefulness-of-hrct-in-screening-of-interstitial-lung-disease-in-patients-with-systemic-sclerosis-without-risk-factors-of-clinical-suspicion/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/usefulness-of-hrct-in-screening-of-interstitial-lung-disease-in-patients-with-systemic-sclerosis-without-risk-factors-of-clinical-suspicion/