Session Information
Title: Imaging of Rheumatic Diseases I: Imaging in Gout, Pediatric, Soft and Connective Tissue Diseases
Session Type: Abstract Submissions (ACR)
Background/Purpose: Axial (spinal) involvement has become increasingly recognized as a potential manifestation of gouty arthritis. The presentation can vary widely from mild, asymptomatic disease to severe back pain, radiculopathy or frank spinal cord compression. Axial gout is frequently a missed diagnosis for a variety of reasons: it can mimic other spine diseases, is under-recognized as a possible manifestation of gout, and current imaging techniques (X-ray, MRI and CT) often produce non-specific findings which do not distinguish gouty erosions and tophi from other pathologies.
Dual-energy CT has recently been recognized as very sensitive and specific for identifying monosodium urate (MSU) crystal deposition. By using a specific display algorithm that assigns different colors to materials of different chemical composition, MSU can be color-coded and thereby distinguished from surrounding structures. Up until now, it has been used mainly to image peripheral sites but has not been evaluated as a diagnostic tool for axial gout.
Methods: We present two cases that demonstrate the efficacy of dual-energy CT in detecting MSU deposition within the axial skeleton. Patient X was a 91 year-old male with severe neck pain, fevers and leukocytosis. MRI showed abnormal T2 signal around the C4-C5 facet joint with fluid consistent with synovitis. However, septic arthritis could not be ruled out. The patient also complained of right knee pain and swelling. Aspirate of the knee revealed intracellular MSU crystals with negative cultures, consistent with acute gout flare. This raised suspicion that the patient’s presentation could be secondary to spinal involvement of gout. Patient Y was a 29 year-old male with a long-standing history of chronic tophaceous gout who presented with incapacitating mid-low back pain. Traditional CT showed extensive subchondral erosions throughout the lumbar spine and right sacroiliac joint.
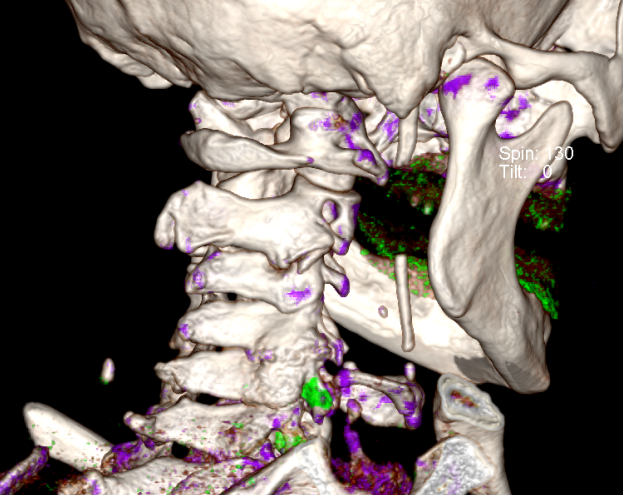
Results: Dual-energy CT of the cervical spine of Patient X (Image 1) showed MSU deposition on the cervical facet joints (color-coded in green) which correlated with the MRI findings. The patient’s symptoms quickly resolved with colchicine and IV methylprednisolone. Similarly, lumbar spine dual-energy CT of Patient Y (Image 2) showed extensive MSU deposition along the transverse processes and pelvic bony structures. Symptoms remitted with colchicine and oral prednisone.
Conclusion: Dual-energy CT can be used to visualize the presence of axial MSU deposition. This may lead to appropriate diagnosis and management of axial gout while avoiding invasive procedures and erroneous treatment.

Disclosure:
K. Logee,
None;
R. Mandhadi,
None;
W. Traverse,
None;
S. Lakshminarayanan,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/use-of-dual-energy-computed-tomography-in-evaluation-of-axial-gout/