Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
Previous publications have suggested that patients in clinical
remission with residual ultrasound (US) synovitis flare more often and do not
stay in remission as long as those without residual US synovitis[1].
Those studies have been performed in single centers by a few highly skilled
operators. Before recommending the use of US as a predictor of flare in daily
practice, those observations need to be confirmed in real life studies.
The objective of this study was to investigate the predictive
value of US residual synovitis on loss of remission in a national cohort of
patients followed in real life by many different rheumatologists operating on
many different US machines
Methods: US significant residual synovitis has been defined
on the Swiss SONAR score, which adopted the single joint definition of
pathologies according to OMERACT for 22 joints. Recently, the SONAR score was
validated against clinical disease activity parameters and the ACR/EULAR
remission status in a large cross-sectional setting among patients in the Swiss
RA registry (SCQM) [2]. For each patient we identified the first visit in
clinical remission (defined as a DAS28 < 2.6) belonging to the first
remission phase during which an assessment of residual US synovitis was
available as the baseline and analyzed time to relapse during follow-up.
Relapse was defined as a DAS28 >= 2.6, start of a biologic, start of an
sDMARD, or start of glucocorticosteroid (GC) therapy or an intensification of
GC therapy, whatever occurred first.
Results:
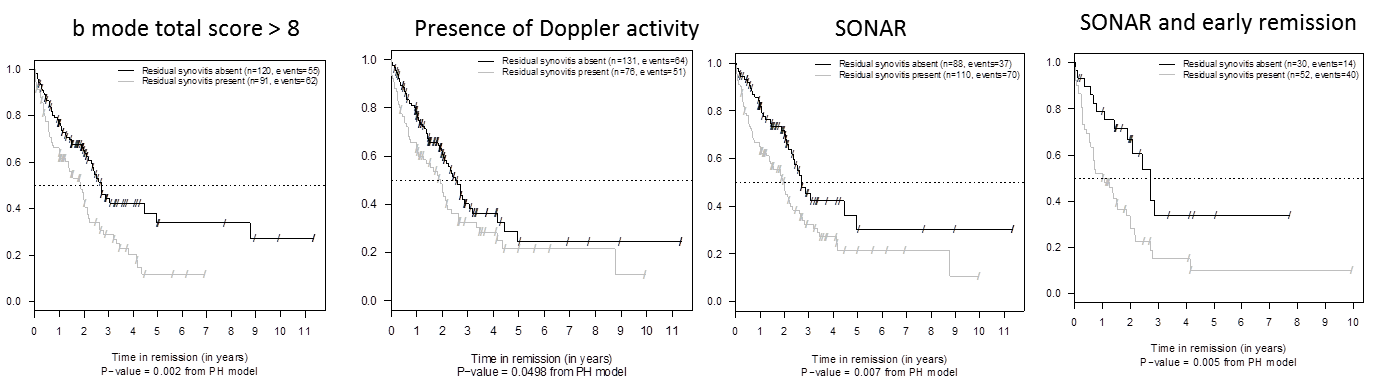
Up to 211 RA patients had US synovitis data and a follow-up. The
majority of patients received a biological treatment at baseline. Significant
residual US synovitis was present in 110 of 198 patients based on SONAR and in
91 of 211 patients considering only b and in 76 of 207 considering only Doppler
mode for defining residual synovitis. Median time to relapse was 2 yrs
(95% CI: 1.4, 2.6) for SONAR+, and 2.7 yrs (95% CI: 2.4, not estimable) for
SONAR-. When we restricted the analysis to the 82 patients who were known to
have been in remission for at most 6 months at baseline (confirmed early
remission), median times to relapse were 1 year (95% CI: 0.7, 2) for SONAR+ and
2.7 yrs (95% CI: 2.1, not estimable) for SONAR-. The same conclusions were
obtained with b or Doppler mode only defined residual synovitis. The figure
displays Kaplan-Meier plots of time to relapse for SONAR+ and SONAR- (all
patients and subgroup of confirmed early remission patients) and for b mode and
Doppler mode only defined residual synovitis.
Conclusion:
Our study in real life patients supports the earlier finding that
residual US synovitis is predictive of duration of remission in RA in particular
in early remission.
References 1 : Rheumatology . 2014
Nov;53(11):2110-8, 2: Joint Bone Spine. 2014 Oct;81(5):426-32
To cite this abstract in AMA style:
Zufferey P, Riek M, Tamborrini G, Brulhart L, Toniolo M, Blumhardt S, Moeller B, Ziswiler HR. Ultrasound Residual Synovitis Has an Impact on the Time to Relapse in RA Patients Considered in Clinical Remission: A Real Life Study of 211 Patients [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/ultrasound-residual-synovitis-has-an-impact-on-the-time-to-relapse-in-ra-patients-considered-in-clinical-remission-a-real-life-study-of-211-patients/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ultrasound-residual-synovitis-has-an-impact-on-the-time-to-relapse-in-ra-patients-considered-in-clinical-remission-a-real-life-study-of-211-patients/