Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Lung involvement is the leading cause of death in systemic sclerosis (SSc) (1). Pulmonary function tests (PFTs) and chest high-resolution CT scan (HRCT) are used to confirm this common complication.
We performed high resolution musculoskeletal (MSK) ultrasound of the nailbed to assess digital clubbing and attempted to correlate with the presence of scleroderma-related interstitial lung disease (SSc-ILD).
Since Hippocratic times, digital clubbing has been described in patients with hypertrophic osteoarthropathy (2), associated with many chronic illnesses such as cardiovascular and pulmonary diseases (3). Digital clubbing is associated with abnormal proliferation of skin and periosteal tissues of the fingertips characterized by periostosis of tubular bones, uniform swelling of soft tissues of the terminal phalanx and increased nail-to-nail bed angle (4). The increased nail bed matrix thickening (NBMT) is associated with digital clubbing, normal reported 1.7+/-0.18mm (5). Our hypothesis is that measurement of the NBMT by MSK Ultrasound can be an effective marker for clinically significant SSc-ILD.
Methods: In this IRB-approved study, we evaluated the dominant hand of 47 subjects by MSK ultrasound. Twenty-nine patients met the 2013 ACT criteria for SSc (6) and were divided into 2 subgroups (Group 2A with ILD and Group 2B without ILD). Eighteen subjects served as the age-matched control group (group 1, no SSc). Using the Phillips Epiq 5, all subjects underwent MSK ultrasound of the dominant hand utilizing linear high frequency probe with 2-22 MHz frequency. The NBMT of all 5 fingers were examined and 235 nail beds were recorded. SSc-ILD was confirmed by HRCT associated with restrictive pattern on PFTs. We used ANOVA testing to calculate differences between groups and a p-value < 0.05 was statistically significant.
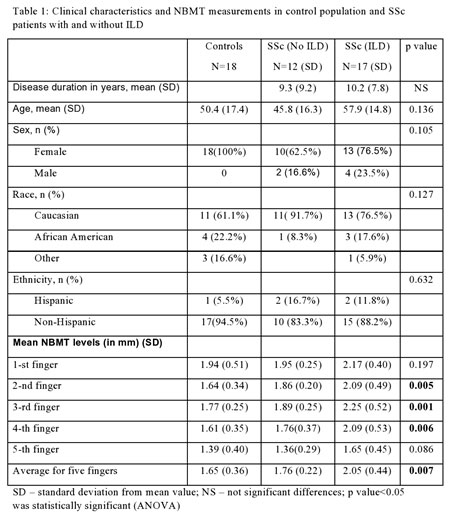
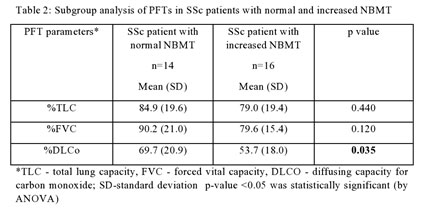
Results: Table 1 shows a significantly higher NBMT for the 2nd, 3rd and 4th fingers in the SSc lung cohort, and inter-digital analysis determined that the 3rd finger NBMT had the highest NBMT between the fingers. The mean cutoff value for normal NBMT in the 3rd finger was less than 2.27mm. The PFT parameters of SSc cohort (Table 2) showed a trend towards increased NBMT in those with SSc-ILD, although only %DLCo was significant in our small cohort.
Conclusion: Our study suggests common mechanisms that may be responsible for digital clubbing in SSc resulting from chronic local tissue hypoxia due to chronic lung disease (7). This is readily visible by MSK ultrasound, often before it is evident on physical exam and may be a predictor of more clinically significant pulmonary disease. We found that a NBMT greater than 2.27mm in the 3rd finger was associated with presence of SSc-ILD. Larger studies are needed to verify our findings.
References:
1. Steen et al: Ann Rheum Dis. 2007; 66: 940
2. Lyons et al: Medicine: An Illustrated History; 1978
3. Martinez-Lavin et al: Semin Arthritis Rheum. 2007; 36:380
4) Martinez-Lavin: Curr Opin Rheumatol. 1997; 9: 83
5) Mondal et al: Rhaumatol Int. 2018;38: 2087
6) Van Den Hoogen et al: Arthritis Rheum. 2013; 65:2737
7) Fomin V et al: Klin Med 2007; 85: 64

Ultrasound 2D Mode -long axis view- of the third finger’s distal phalanx in two SSc subjects with normal -top- and abnormal -bottom- nail bed matrix thickness -NBMT-. Red line represents the NBMT, measured distance between volar plate of the nail and dorsal surface of the distal phalanx bone.
To cite this abstract in AMA style:
Sidor M, Zuckerman R, Schlesinger N, Sussman R, Sabahath H, Hsu V. Ultrasound Measurement of the Nail Bed Matrix Thickness as a Useful Marker for Scleroderma-Related Interstitial Lung Disease [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/ultrasound-measurement-of-the-nail-bed-matrix-thickness-as-a-useful-marker-for-scleroderma-related-interstitial-lung-disease/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ultrasound-measurement-of-the-nail-bed-matrix-thickness-as-a-useful-marker-for-scleroderma-related-interstitial-lung-disease/