Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Methotrexate (MTX) is commonly used in the treatment of children with juvenile idiopathic arthritis (JIA), and intolerance to the drug frequently leads to discontinuation due to anticipatory and associative gastrointestinal symptoms. Eye Movement Desensitization and Reprocessing (EMDR) is a psychotherapy which has been successfully used in MTX intolerance, however with diminishing efficacy over time. BLAST (bi-lateral alternating stimulation tactile) armbands utilize a similar process to EMDR and have already been used in conjunction with this method.
The aim of this study was to determine if utilization of BLAST armbands could improve and prolong the effect of EMDR on patients with MTX intolerance.
Methods: Consecutive patients admitted to the German Center for Pediatric and Adolescent Rheumatology from October 2016 until March 2023 were included in this study. Inclusion criteria were 1) diagnosis of JIA according to ILAR criteria, 2) age between 8 and 17 years, 3) symptoms of MTX intolerance using the Methotrexate Intolerance Severity Score (MISS) questionnaire and 4) necessity of MTX treatment for at least 6 more months as determined by the treating physician. The standard 8 phase EMDR protocol was adapted for the treatment of MTX intolerance. Treatment started with a structured psychosocial and medical history. Subsequently, five sessions lasting 60 minutes each were held over a time period of 10 – 12 days, concluding with an application of MTX in a clinical setting. The initial 50 patients were treated only with EMDR, as previously published (Höfel et al. Pediatric Rheumatology (2018) 16:11). Subsequent patients were treated with EMDR and BLAST armbands which patients continued to use after the initial treatment sessions.
Health-related quality of live was determined using the PedsQL. Measurements of MISS and PedsQL were taken at 4 time points: directly before and after (MISS only) treatment, as well as 4 and 12 months after treatment. Changes in MISS and PedsQL were compared using descriptive statistics and repeated measures ANOVA.
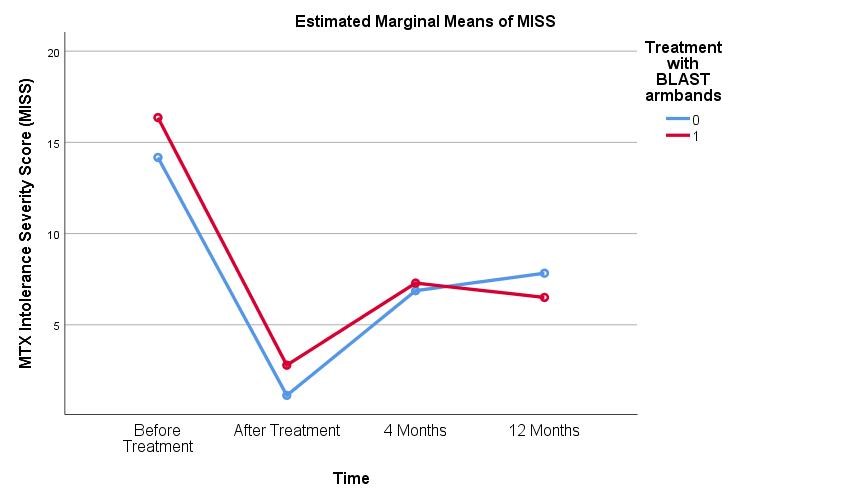
Results: 93 patients with MTX intolerance [median MISS at inclusion: 14 (range 6 – 26)] were included, 50 in group 1 without BLAST armbands and 43 in group 2 which were concurrently treated with BLAST armbands. Directly after treatment, all patients reported marked improvement of MTX intolerance symptoms [group 1: median MISS: 1 (0 – 6), group 2: median MISS: 2 (0 – 11)]. Four months after treatment, median MISS score in group 1 was 5.5 (0-26), and 5 (0-25) in group 2. After 12 months median MISS was 8 (0-33) in group 1, and 6 (0-17) in group 2. A repeated measures ANOVA showed a significant difference between the MISS results (F(3,105) = 53.7, p = .000). Median quality of life as measured by the PedsQL rose after 12 months from 79.4 to 87.0 in group 1, and from 72.7 to 91.3 in group 2.
Conclusion: Treatment with Eye Movement Desensitization and Reprocessing (EMDR) presents an effective treatment of MTX intolerance, and further significant improvement can be achieved using BLAST armbands. This can facilitate continuation of MTX treatment in patients with MTX intolerance and has the potential to significantly increase quality of life in affected children.
To cite this abstract in AMA style:
Höfel L, Eppler B, Haas J, Hugle B. Treatment of Methotrexate Intolerance in Juvenile Idiopathic Arthritis Using Eye Movement Desensitization and Reprocessing (EMDR) Can Be Improved by Bi-lateral Alternating Stimulation Tactile (BLAST) Armbands [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/treatment-of-methotrexate-intolerance-in-juvenile-idiopathic-arthritis-using-eye-movement-desensitization-and-reprocessing-emdr-can-be-improved-by-bi-lateral-alternating-stimulation-tactile-blast/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treatment-of-methotrexate-intolerance-in-juvenile-idiopathic-arthritis-using-eye-movement-desensitization-and-reprocessing-emdr-can-be-improved-by-bi-lateral-alternating-stimulation-tactile-blast/