Session Information
Date: Sunday, November 10, 2019
Title: 3S078: RA – Diagnosis, Manifestations, & Outcomes I: Pulmonary & Other Comorbidities (839–844)
Session Type: ACR Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Multimorbidity, the presence of multiple chronic conditions, predisposes individuals to disability and premature mortality. RA is well known to be associated with select chronic conditions, but the timing of onset of multimorbidity and the rate of accruing additional conditions is not well established. We aimed to determine the trajectory of multimorbidity in RA compared to the general population.
Methods: We assembled RA cohorts within Truven MarketScan database from 1/2006-9/2015 using ≥2 ICD-9 codes for RA, a rheumatologist diagnosis, and DMARD use. Incident RA was identified using validated algorithms for claims data that required at least 12 months of observable time with medical and pharmacy coverage (observability) without RA diagnostic codes or DMARDs (Curtis et al. AC&R, 2018). RA subjects were matched 1:1 to non-RA subjects on age, sex, and calendar year. Chronic conditions were identified from observability to the end of follow-up (censoring at disenrollment or end of study period) using ICD-9 codes for 48 chronic conditions identified in systematic reviews of multimorbidity. Conditions occurring on or before the date fulfilling the RA algorithm (or equivalent date for non-RA) were considered prevalent. Multimorbidity was defined as having ≥2 chronic conditions (not including RA) and multimorbidity burden was defined by the number of conditions present. Cross-sectional prevalence and burden of multimorbidity in all RA vs. non-RA was determined using conditional logistic and negative binomial regression. The trajectory of multimorbidity over time in incident RA vs. non-RA was assessed using generalized estimating equations with an interaction term between RA status and year of follow-up.
Results: A total of 139,403 RA subjects (overall cohort) were matched to 139,403 non-RA subjects. This included a subcohort of 30,764 incident RA subjects. Mean (SD) age was 54.1 (13.4) years with 76.5% female. Time from observability to index date was 1.2 (1.8) years in the overall group and 3.2 (1.9) years in the incident subcohort. In the overall cohort, multimorbidity was present in 34.2% of RA subjects vs. 21.3% of non-RA (OR 2.30, 95% CI 2.26-2.35, p< 0.001). Multimorbidity burden was significantly higher in RA vs. non-RA (ratio of conditions 1.67, 95% CI 1.65-1.69, p< 0.001). Of the 48 chronic conditions examined, 42 were overrepresented (Table 1). In the incident subcohort, multimorbidity frequency was higher in RA subjects throughout follow-up (OR 2.75, 95% CI 2.66-2.84). Similarly, multimorbidity burden was higher in incident RA than non-RA at baseline and throughout follow-up (Figure 1; ratio of conditions 1.76, 95% CI 1.73-1.79). The rate of accruing chronic conditions was not higher in incident RA than non-RA (ratio of accruing conditions per year 0.99, 95% CI 0.98-1.00, p=0.06).
Conclusion: In a large, national, commercial claims database, we found the odds of multimorbidity were 2.3-fold higher in RA compared to the general population. Trajectory analyses in those with new onset disease suggest the heightened risk of multimorbidity in RA occurs early in the disease course or may even precede RA onset.
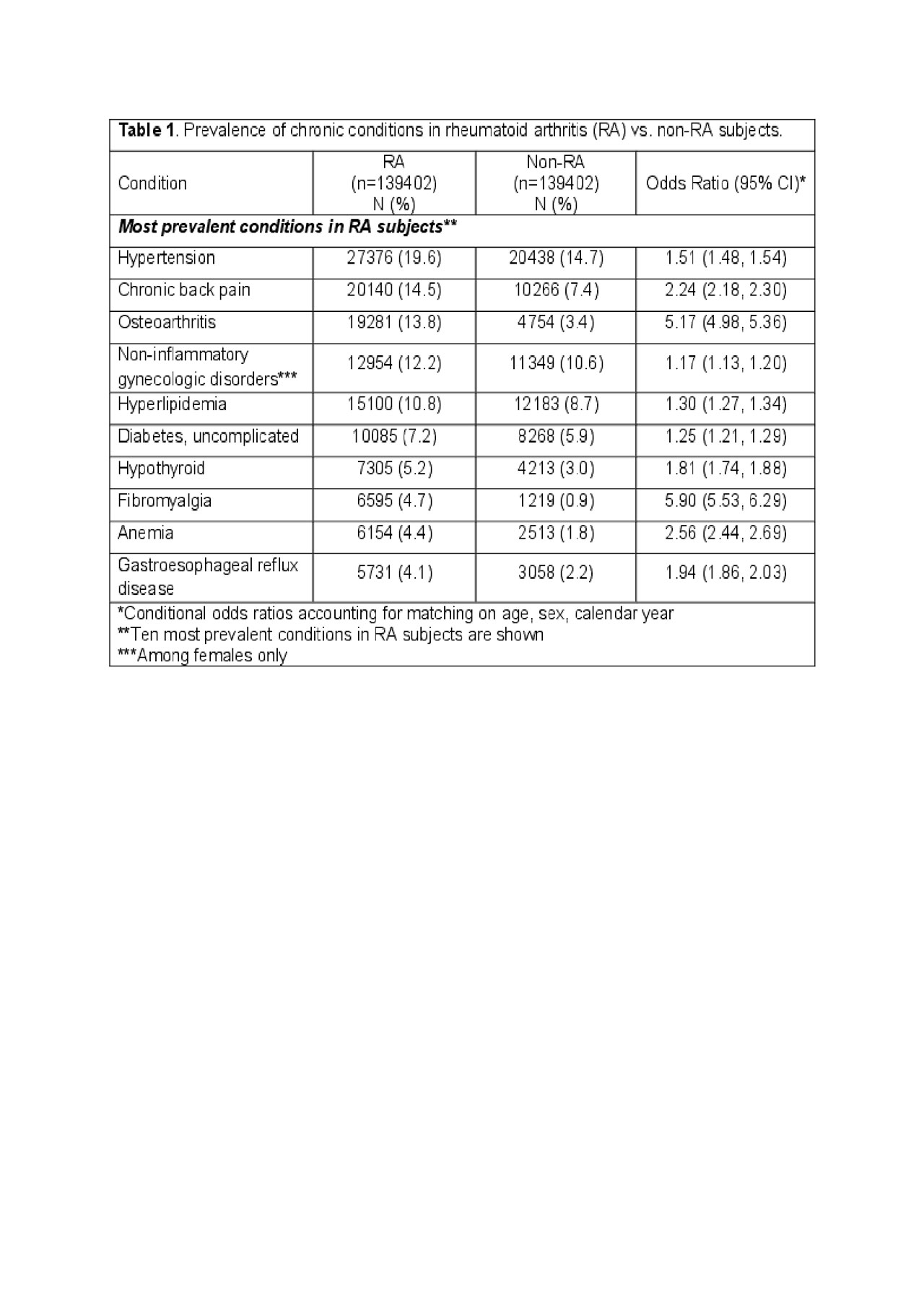
Table 1 RA multimorbidity trajectory_20190529
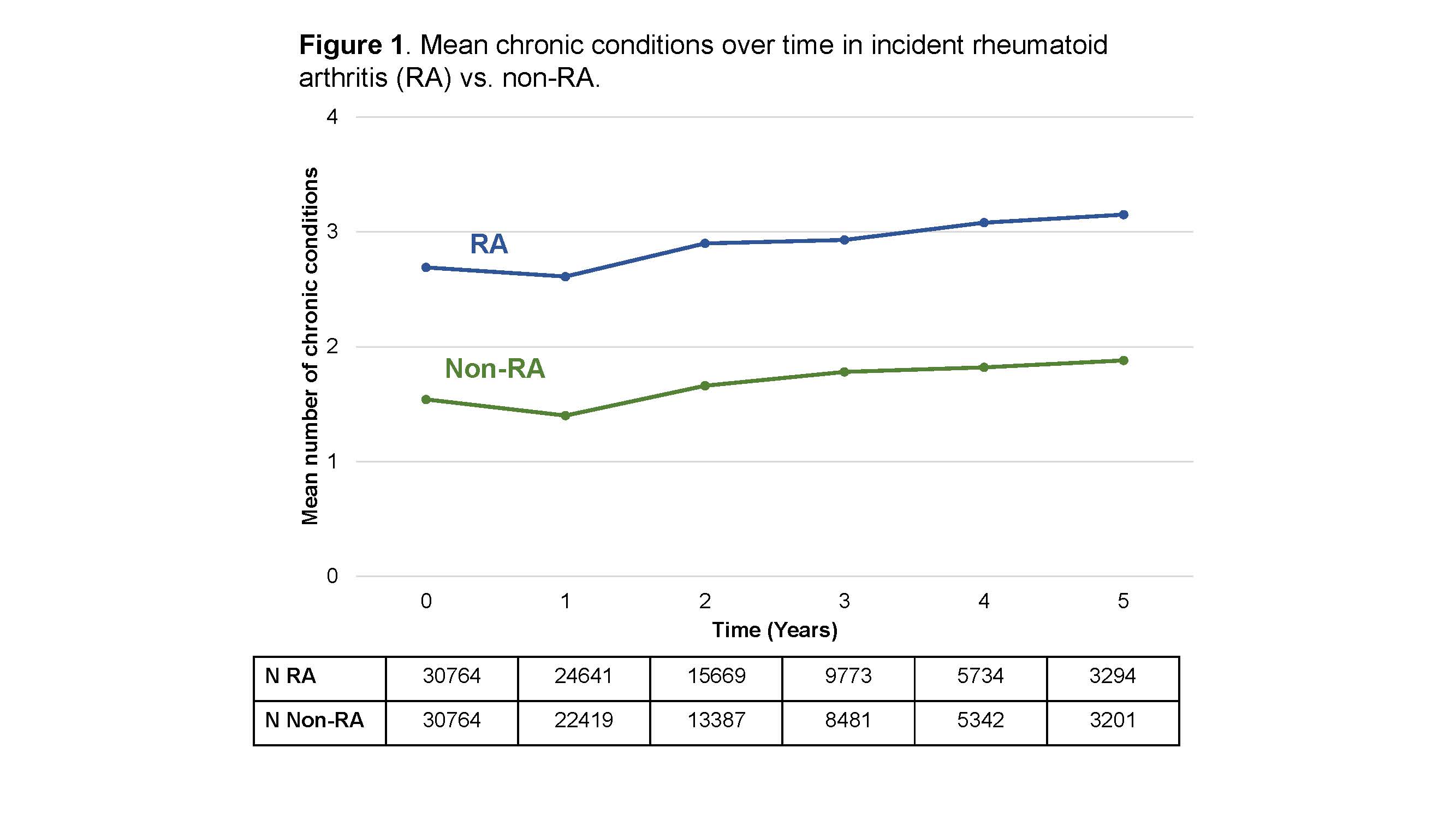
Figure 1 RA multimorbidity trajectory_20190529
To cite this abstract in AMA style:
England B, Roul P, Yu F, Sayles H, Michaud K, Xie F, Curtis J, Mikuls T. Trajectory of Multimorbidity in Rheumatoid Arthritis in a U.S. Commercial Insurance Claims Database from 2006-2015 [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/trajectory-of-multimorbidity-in-rheumatoid-arthritis-in-a-u-s-commercial-insurance-claims-database-from-2006-2015/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/trajectory-of-multimorbidity-in-rheumatoid-arthritis-in-a-u-s-commercial-insurance-claims-database-from-2006-2015/