Session Information
Date: Sunday, November 13, 2016
Title: Rheumatoid Arthritis – Clinical Aspects - Poster I: Clinical Characteristics/Presentation/Prognosis
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: The elbow is an easily-examined joint and an important determinant of morbidity in rheumatoid arthritis (RA). In active RA the measured elbow extension angle, recorded as degrees of flexion, consists of the sum of a fixed (irreversible destruction) deficit and a functional deficit (potentially reversible by medical or physical therapy). In inactive RA, the angle approaches the fixed, irreversible baseline. One of us (Case) has been measuring the angle and obtaining the DAS28-CRP(4) as part of routine clinical care. We undertook a 3-year retrospective study (5/1/12 – 4/31/15) of RA patients in order to determine a relationship between disease activity and the elbow extension angle.
Methods: All RA patients seen during the first (recruitment) year of study were eligible if they had RA (ACR/EULAR criteria), had at least 4 visits, had at least 3 elbow and DAS determinations and at least one of each during the first and last 3 visits. A Grafco 12-1000 Orthopedic goniometer (GF Health Products, Atlanta GA) was used in all measurements. After determining the high (< 0.0001) correlation between right and left elbow extension angles, the sum (right plus left, in degrees of flexion, “ELB”) was used for statistics. A baseline best ELB (i.e., lowest flexion contracture) was determined from the first 3 visits and a final from the last 3 visits up to and including visit 10 (after which patient numbers rapidly dropped off precluding statistics). 166 patients entered into the study. 23 were subsequently excluded. Correlation was assessed by Pearson, and group differences between remitters (defined as DAS < 2.6) and non-remitters (defined as DAS >= 2.6) were assessed by T-test. Statistics were calculated with IBM SPSS 22.
Results: The 143 patients had a mean age of 53.2 (SEM 13.2) years (122 females and 21 males). Patients were followed for a mean of 28.4 (SEM 6.6) months over a mean of 8.68 (SEM 2.41) visits. Because the best (i.e., lowest) mean ELB occurred between the 3rd and 4th visits, we conservatively chose the 4th visit in comparison with the 10th visit for statistical comparison (see Figure). Between visits 4 and 10 ELB increased from 19.3 (SEM 3.91) to 23.3 (SEM 5.91) (4.0 degrees) for non-remitters and from 1.96 (SEM 1.23) to 2.70 (SEM 2.38) (0.74 degrees) for remitters, a greater than 5-fold difference (p<0.0001). Correspondingly, the difference between the 4th and 10th visits for non-remitters was significant (p<0.001) but for remitters was not (p=0.264). The Figure shows all patients (___, middle line) and that remitters (_._., lower line) maintained ELB over the course of the study, while non-remitters (_ _ _, upper line) did not. Non-remitters also had a higher baseline ELB than remitters (p<0.0001). 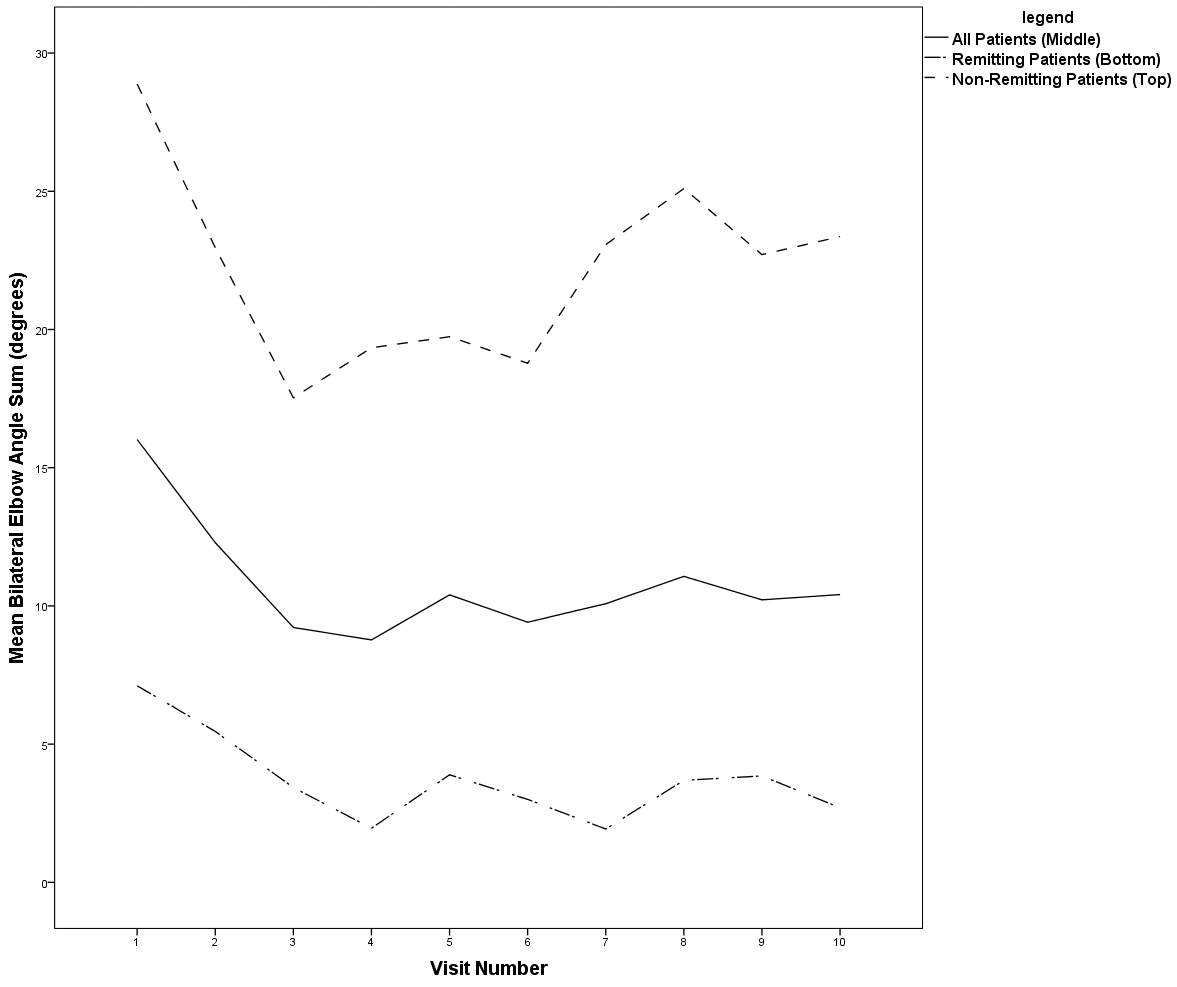
Conclusion: The ELB closely correlates with disease activity. DAS non-remitters had a five-fold poorer ELB outcome than DAS remitters. Measurement of the ELB may be an important supplement to the rheumatologic exam in clinical and research settings.
To cite this abstract in AMA style:
Case JP, Wang C, Tucker H. The Summed Bilateral Elbow Extension Angle in Rheumatoid Arthritis Correlates with the DAS28-CRP(4) and May be an Independent Marker of Bad Prognosis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/the-summed-bilateral-elbow-extension-angle-in-rheumatoid-arthritis-correlates-with-the-das28-crp4-and-may-be-an-independent-marker-of-bad-prognosis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-summed-bilateral-elbow-extension-angle-in-rheumatoid-arthritis-correlates-with-the-das28-crp4-and-may-be-an-independent-marker-of-bad-prognosis/