Session Information
Date: Monday, November 13, 2023
Title: Abstracts: Vasculitis – Non-ANCA-Associated & Related Disorders I: Imaging
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: GCA is a systemic medium-large vessel vasculitis (M-LVV) involving the cranial arteries, aorta and its major branches. Recent studies have shown that PET/CT including the cranial and large vessels offers high diagnostic accuracy for GCA in research settings. At our institution in Sydney, Australia, PET/CT is the protocolized first-line investigation for GCA, and here we report its diagnostic performance in this “all comer” real world setting.
Methods: We audited all inpatients and outpatients investigated with PET/CT for suspected new onset GCA between July 2019 and March 2022. Patients were scanned from vertex to thighs with arms by their side, 90 minutes post-fluorodeoxyglucose (FDG) administration. Patients completed a self-reported questionnaire at the time of scan. Scans were reported by the experienced nuclear medicine physician of the day as overall positive, equivocal or negative for M-LVV. FDG uptake by vascular region was also reported. The gold standard comparator was the treating clinician’s diagnosis of active M-LVV at a minimum of 6 months post the time of the scan. Active M-LVV included diagnoses of GCA, large vessel vasculitis and aortitis. Temporal artery biopsy (TAB) and vascular US results conducted within 4 weeks of scan were recorded.
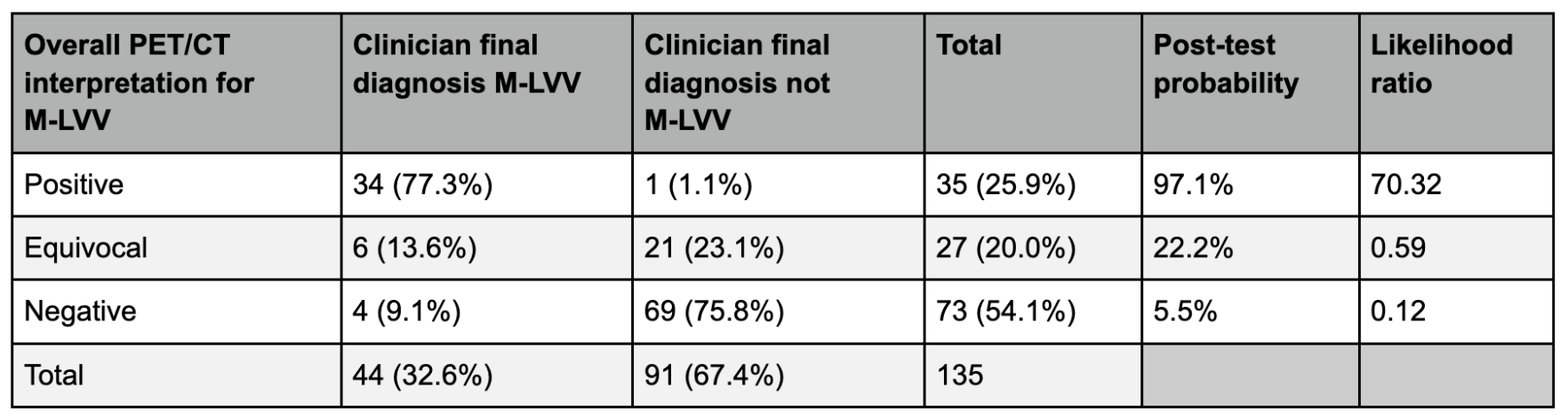
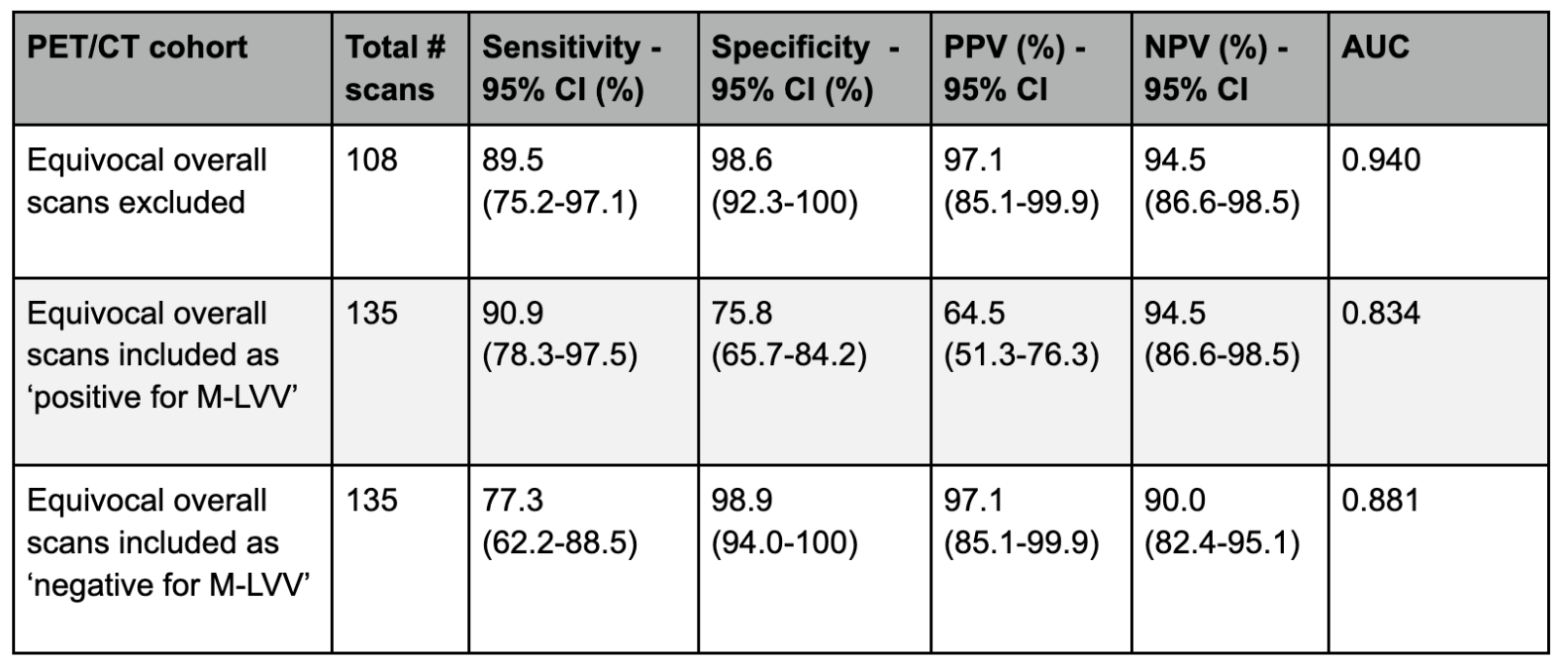
Results: 135 patients underwent PET/CT for suspected new onset GCA, with a median age of 73 years (range 48-98), 70% were female. 86 (63.7%) patients were taking glucocorticoids at the time of scan. 44 (32.6%) patients had a final clinical diagnosis of active M-LVV. 35 (25.9%) scans were reported as positive, 27 (20%) equivocal and 73 (54.1%) negative for M-LVV. The likelihood ratio for a diagnosis of active M-LVV with a positive scan was 70.3, equivocal scan 0.59, and a negative scan 0.12. Sensitivity (Sn) and specificity (Sp) of PET/CT was dependent on treatment of equivocal scans in the binary analysis. If equivocal scans were excluded, Sn was 89.5% and Sp 98.6%. If equivocal scans were considered positive, Sn was 90.9% and Sp 75.8%. If equivocal scans were considered negative, Sn was 77.3% and Sp 98.9%. 55/135 (40.7%) patients underwent TAB and/or US (27 TAB, 33 US, 5 both TAB and US) as an additional investigation to PET/CT. 13/55 (23.6%) in this cohort had equivocal PET/CT scans, and 11/13 of the additional test (TAB/US) results matched the clinical diagnosis. In the total cohort, TAB had a Sn of 42.9% and Sp of 100%, and US had a Sn range of 53.3% to 66.7% (dependent on treatment of the 2 equivocal US) and Sp of 88.9%. For the 34 patients with positive PET/CT scans and a clinical diagnosis of M-LVV, significant FDG uptake was most commonly reported in the supra-aortic (88.2%), followed by cranial (55.9%), aortic (52.9%) and infra-aortic (23.5%) regions.
Conclusion: This is the largest real-world study of combined cranial and large vessel PET/CT as a first-line test for GCA. PET/CT had good diagnostic performance with sensitivity ranging from 77.3 to 90.9%, and specificity 75.8 to 98.9% for a clinician diagnosis of active M-LVV, dependent on treatment of equivocal scans. TAB and/or US can be used as ancillary tests to help confirm a diagnosis when PET/CT is indeterminate or discordant with the clinical presentation.
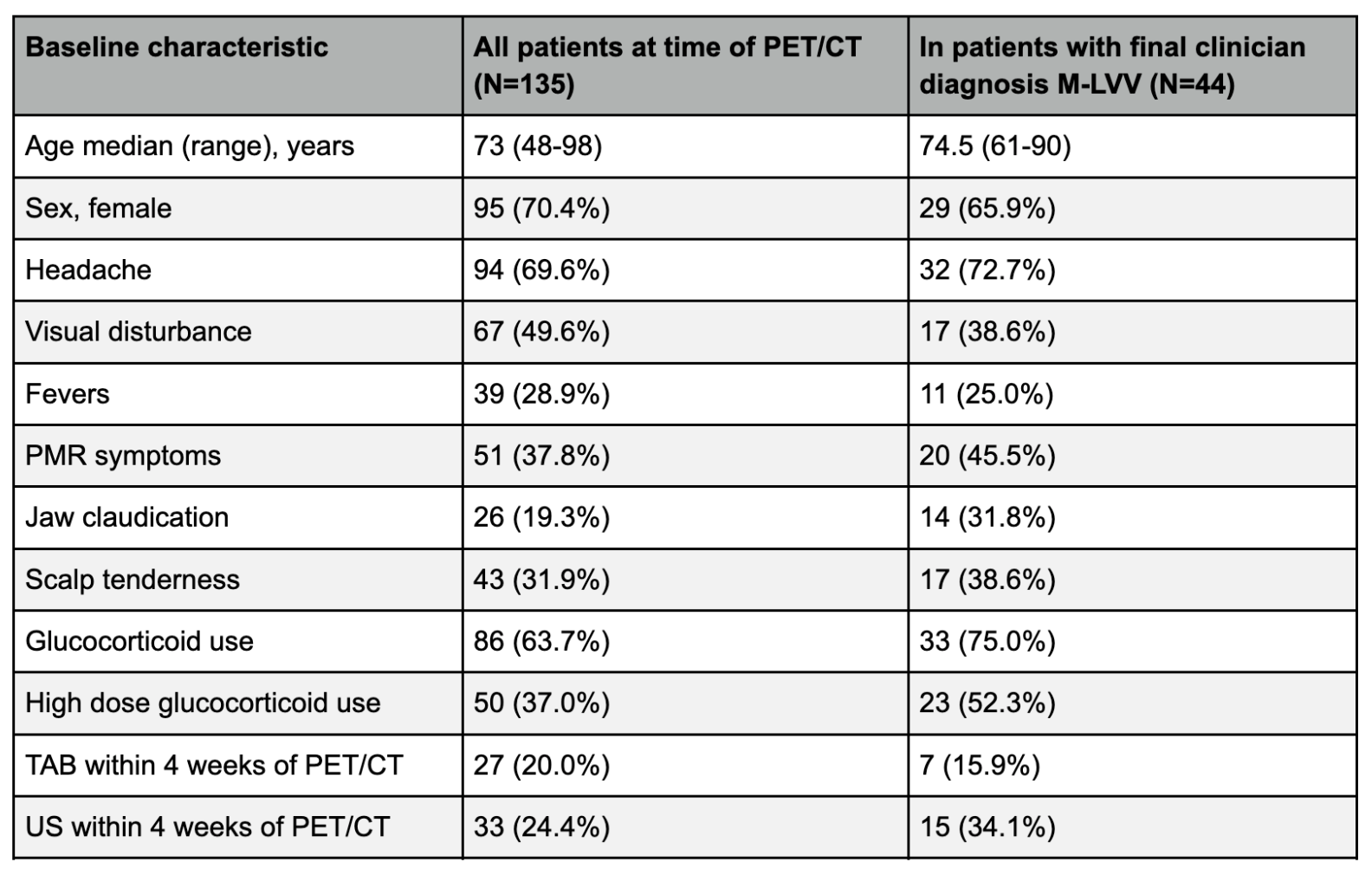
Values are number (%) of patients, except where indicated otherwise
PMR = polymyalgia rheumatica
TAB = temporal artery biopsy
US = vascular ultrasound temporal +/- axillary arteries
High dose glucocorticoid use = prednisone ≥40mg oral daily or methylprednisolone ≥500mg IV daily
M-LVV = medium-large vessel vasculitis
M-LVV = medium-large vessel vasculitis
PPV = positive predictive value
NPV = negative predictive value
CI = confidence interval
AUC = area under the receiver operating curve
To cite this abstract in AMA style:
Port K, Ho Shon I, Ayesa S, Langford R, Bennett O, Csillag A, Fredericks S, Palacios-Derflingher L, Wegner E, Sammel A. The Real-World Experience of Combined Cranial and Large Vessel FDG-PET/CT in the Investigation of Giant Cell Arteritis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/the-real-world-experience-of-combined-cranial-and-large-vessel-fdg-pet-ct-in-the-investigation-of-giant-cell-arteritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-real-world-experience-of-combined-cranial-and-large-vessel-fdg-pet-ct-in-the-investigation-of-giant-cell-arteritis/