Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: The prevalence and incidence of Behcet’s syndrome (BS) in the UK is unknown at an unselected population level. BS may be associated with phenotypically related MHC class 1 conditions yet there are no UK based studies underpinning this association or assessing diagnostic delay in BS. CPRD and linked HES provide a national resource to further explore the epidemiology of BS in a non-endemic western population
Objectives:
- Annual incidence rate and prevalence per million person years will be calculated stratified by age, sex, ethnicity and area-based deprivation
- Risk factors for BS: age, smoking, obesity, ethnicity, gender, socio-economic deprivation and presence of phenotypically linked MHC class 1 diseases
- Time to diagnosis of BS from first recorded symptom: oral or genital apthosis, ocular manifestations, cutaneous, neurological, GI, and vascular manifestations
Methods: CPRD (primary care) and linked HES (secondary care) databases were used to estimate yearly point prevalence and incidence rates for BS using read code diagnosis of BS between 2001 to 2021. For those with both HES and CPRD read code of BS, the earliest date was used for diagnosis. A retrospective matched case control study design was used to evaluate BS risk (odds ratio) for a variety of pre-selected covariates of interest. Controls were selected at a 1:10 ratio (age, gender and practice matched). To evaluate the relationship of phenotypically related MHC class 1 conditions at baseline with BS risk in cases versus controls, logistic regression was used to calculate adjusted odds ratios. We estimated median time from first clinical code of a manifestation of interest and CPRD/HES confirmed diagnosis of BS
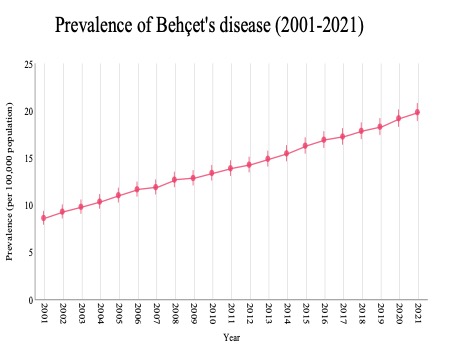
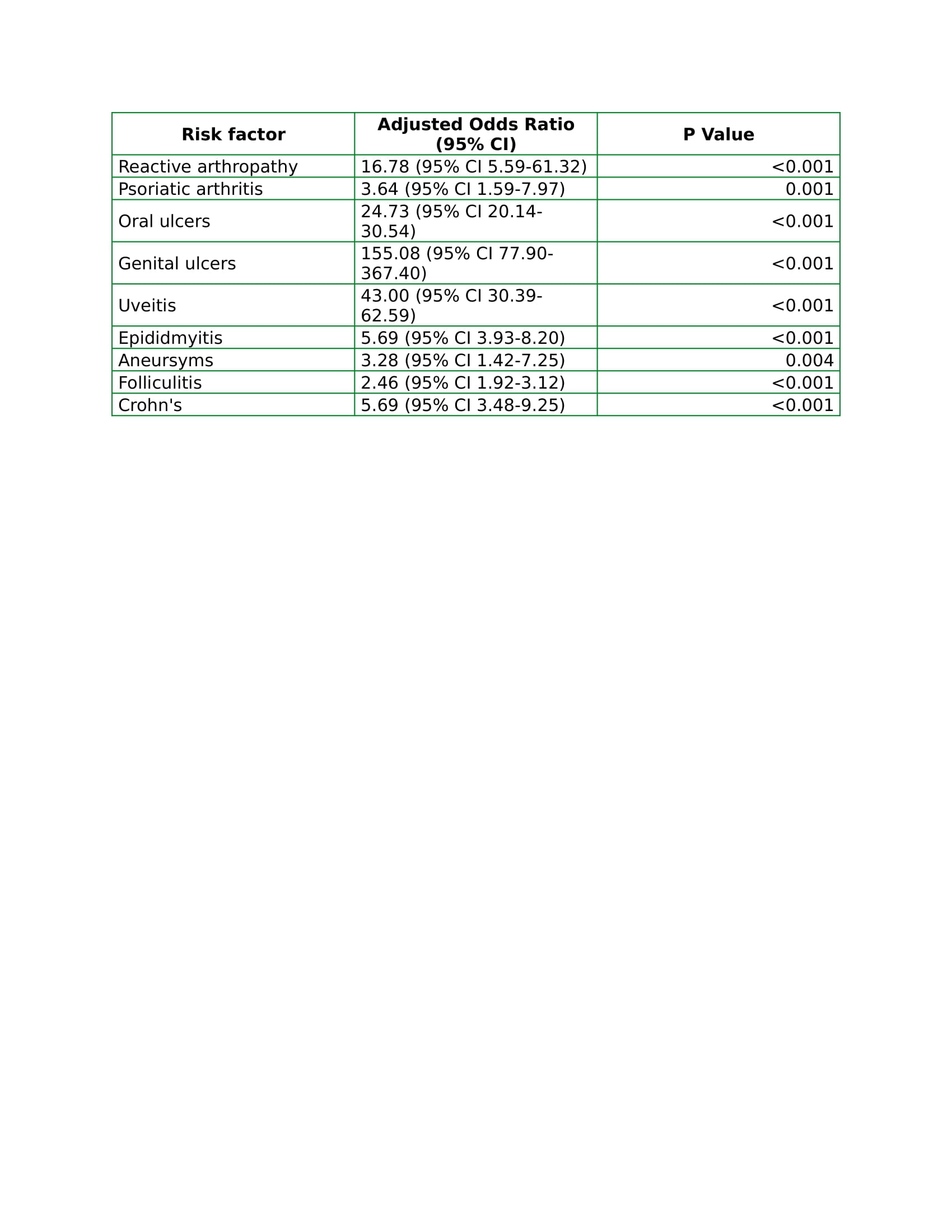
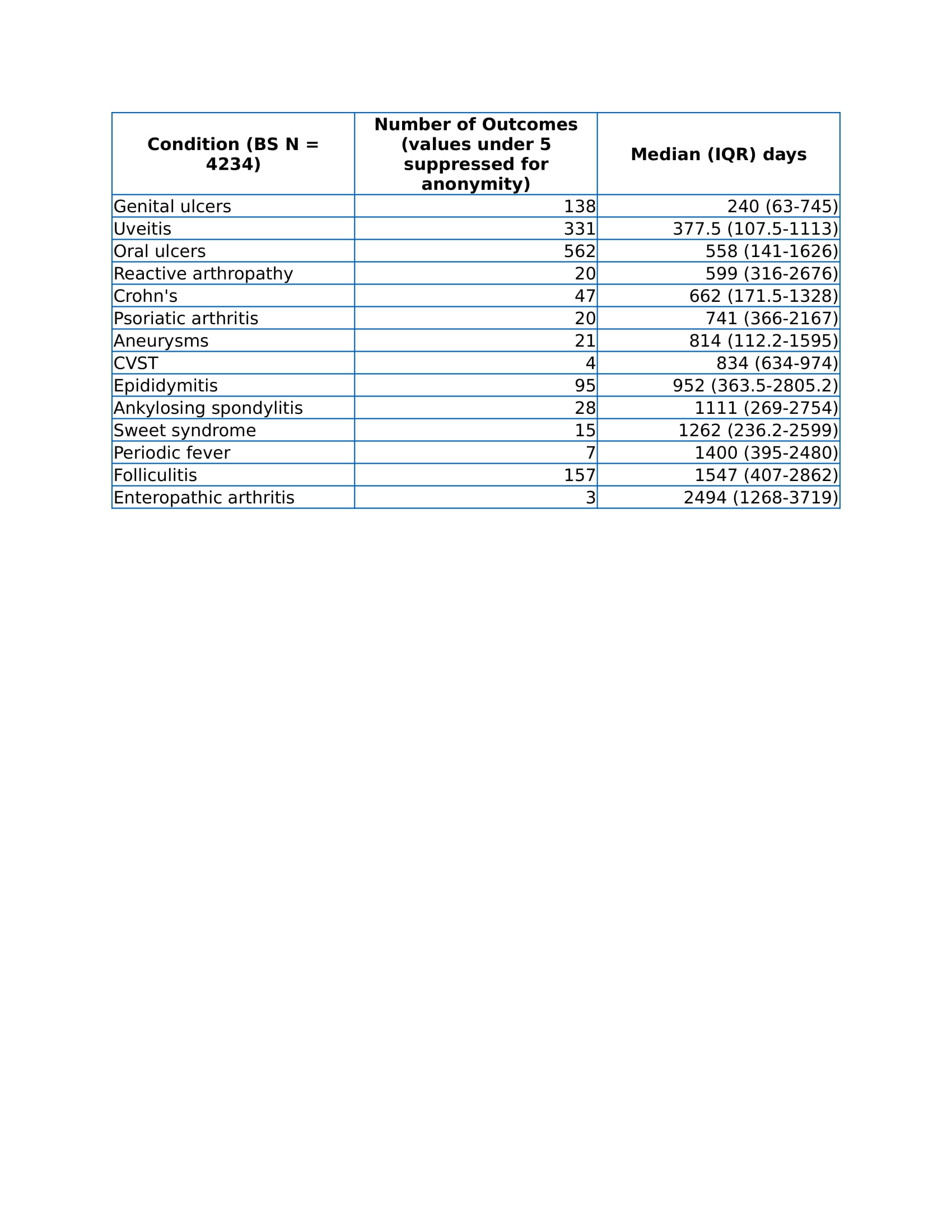
Results: A total of 4810 cases of BS were noted during the study period. Prevalence of BS was 19.07 per 100,000 (95% CI 19.93, 18.23) in 2020, rising compared to previous years (12.5/100,000 in 2006) (fig. 1). Incidence of BS was stable, 0.89 per 100,000 (95% CI 1.09, 0.71). Both prevalence and incidence were highest amongst females, in Southwest England and amongst those of mixed-race ethnicity. Prevalence and incidence were highest amongst the 31 – 40 age group in 2020. A sample of 1752 cases of BS in CPRD were compared with 5716 age and gender matched controls. The strongest association of BS was with the following conditions at baseline (table 1): genital ulceration (OR 88.21 (41.70-221.91), uveitis (OR 28.57 (19.12-44.18) and oral ulceration (OR 27.50 (21.62-35.33) amongst participants with BS compared to controls. A chronological sequence for appearance of phenotypic element leading to a BS diagnosis was established. The shortest median (IQR) time to diagnosis of BS was 240 (63-745) from having the first clinical code for genital ulceration, longest for enteropathic arthritis 2494 (1268-3719) (table 2)
Conclusion: The prevalence of BS appears higher than previously thought in the UK. Misclassification with phenotypically related conditions may be a factor. BS phenotype might have multiple origins through conditions with genetic and phenotypic overlap as risk of BS seems to be increased in those with a genetically linked condition. Evident diagnostic delay can be avoided by increased recognition of key clinical manifestations
To cite this abstract in AMA style:
Chandratre P, Chandan J, Hammond B, Thayakaran R, Cusworth S, Adderley N, Situnayake D. The Prevalence, Incidence, Risk Factors and Time to Diagnosis of Behcet’s Syndrome in England: A Retrospective Nested Case Control Study in Clinical Practice Research Datalink and Hospital Episode Statistics [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/the-prevalence-incidence-risk-factors-and-time-to-diagnosis-of-behcets-syndrome-in-england-a-retrospective-nested-case-control-study-in-clinical-practice-research-datalink-and-hospital-epi/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-prevalence-incidence-risk-factors-and-time-to-diagnosis-of-behcets-syndrome-in-england-a-retrospective-nested-case-control-study-in-clinical-practice-research-datalink-and-hospital-epi/