Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Although concomitant infectious diseases are the predominant causes of death in patients with polymyositis (PM)/dermatomyositis (DM)-associated interstitial lung disease (ILD), intensive immunosuppressive treatment are necessary for severe cases. We have already reported that high initial dose of glucocorticoid for induction therapy, high serum LDH and KL-6 levels at the baseline were independent risk factors for infection. Here we investigated the predictive risk factors for opportunistic infection during treatment for PM/DM-ILD by assessing cytomegarovirus (CMV) antigen test as a barometer for immunocompromised status.
Methods: We retrospectively analyzed clinical features, laboratory data and high-resolution computed tomography (HRCT) findings at baseline in the patients with PM/DM-ILD who had received initial treatment at six hospitals affiliated to Yokohama City University from 2003 to 2016. We also investigated initial therapeutic regimens and clinical outcomes including CMV antigenemia as a complication. We conducted univariate and multivariate analyses to extract risk factors for CMV antigenemia.
Results: One hundred sixteen patients (PM 22, DM 51, and clinically amyopathic DM (CADM) 43) were recruited. The mean age was 56 ± 15 years and 83 (71.6%) were female. As initial therapies, oral prednisolone (PSL) was prescribed in all patients. Methylprednisolone (mPSL) pulse, intravenous cyclophosphamide (IVCY), and oral calcineurin inhibitor therapies were performed in 78 (67%), 48 (41%) and 81 (70%), respectively. Forty patients (34%) received combination therapy with IVCY and a calcineurin inhibitor. Forty-two patients (36%) had CMV antigenemia within 6 months from initiation of immunosuppressants. Low serum albumin and PaCO2 levels (p = 0.001 and p = 0.004, respectively), high serum ferritin levels (p = 0.007), ILD region existing in the upper lung field (p = 0.008), high initial PSL dose (p = 0.006), mPSL pulse (p = 0.001), IVCY (p < 0.001), and combination therapy (p < 0.001) were extracted as risk factors for CMV antigenemia by univariate analyses (Table 1). There were no association between the cumulative PSL dose and CMV antigenemia. A multivariate logistic regression analyses revealed that low PaCO2 (p = 0.044, OR 4.96), above 0.6 mg/kg/day of initial PSL dose (p = 0.027, OR 3.56) and the treatment with oral calcineurin inhibitor (p = 0.007, OR 21.23) were independent risk factors for CMV antigenemia. Of 27 patients who died during the observation period 13 (48%) had CMV antigenemia.
Conclusion: Although rapid and intensive therapies are required for PM/DM- ILD, appropriate monitoring, prophylaxis and early treatment for opportunistic infection are important, especially in patients who receive high initial dose of glucocorticoid or calcineurin inhibitor and who show low PaCO2 level.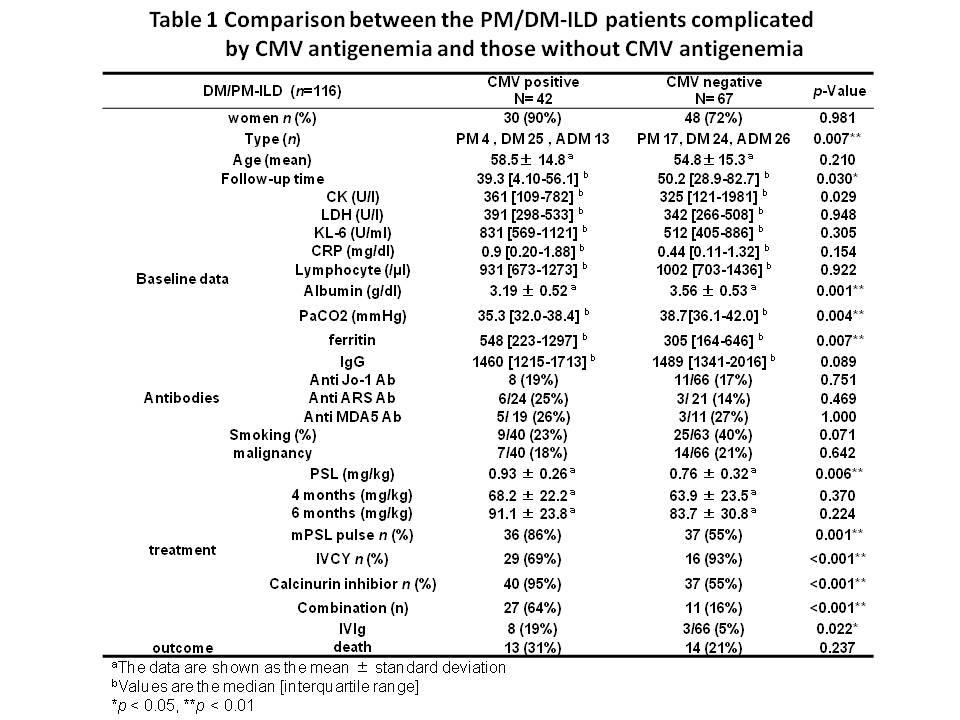
To cite this abstract in AMA style:
Sugiyama Y, Yoshimi R, Tamura M, Hamada N, Nagai H, Tsuchida N, Kunishita Y, Soejima Y, Kishimoto D, Kamiyama R, Minegishi K, Kirino Y, Ohno S, Nakajima H. The Predictive Risk Factors for Opportunistic Infection during Treatment for Polymyositis/Dermatomyositis-Associated Interstitial Lung Disease [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/the-predictive-risk-factors-for-opportunistic-infection-during-treatment-for-polymyositisdermatomyositis-associated-interstitial-lung-disease/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-predictive-risk-factors-for-opportunistic-infection-during-treatment-for-polymyositisdermatomyositis-associated-interstitial-lung-disease/