Session Information
Date: Sunday, November 13, 2016
Title: Rheumatoid Arthritis – Clinical Aspects - Poster I: Clinical Characteristics/Presentation/Prognosis
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: In patients (pts) with rheumatoid arthritis (RA), the American College of Rheumatology (ACR)20 score was developed to best discriminate effective from placebo (PBO) treatment, minimize PBO response rates, assess the efficacy of a drug vs PBO and clinical outcome over a period. Based on trials of pts with established RA and on use of csDMARDs, ACR20 was determined to be the best discriminator vs ACR 50/701. However, it is unclear if ACR20 is also the best discriminator between treatments in studies conducted in the current era. The aim was to determine the cut-off value of the ACR score which can best discriminate between the efficacies of various treatments in RA pts in a clinical trial (CT).
Methods: This post hoc analysis used data from the PREMIER2 and OPTIMA3 CTs in pts with early RA who were methotrexate (MTX) naïve and from the DE0194 and ARMADA5 CTs in pts with established RA who had failed prior DMARD(s). To identify the ACR score with best discrimination between treatments, the ACR response rate was calculated for each treatment arm at various time points for each cut-off from 0-100. The p-value was calculated for the difference between treatments at each cut-off to identify the cut-off for which the p-value was the smallest.
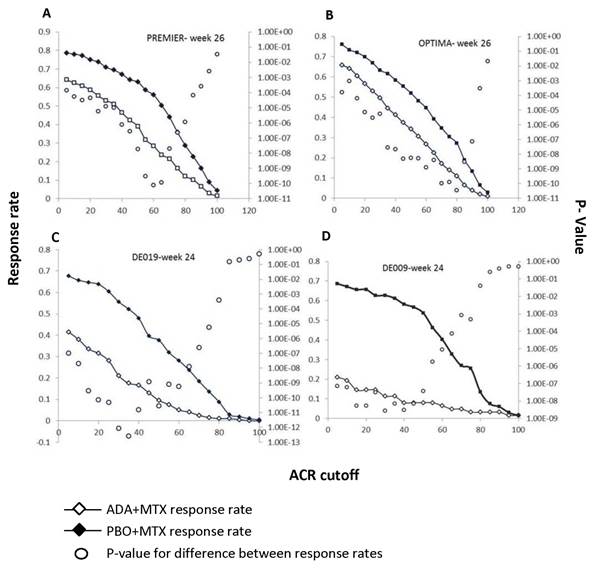
Results: In pts from PREMIER (early RA), the maximum difference and best p-value between the PBO+MTX (newly introduced MTX) vs originator adalimumab (ADA)+MTX arms was achieved at ACR60 (fig 1A) at Week (Wk) 26. Similarly, in OPTIMA (early RA), at Wk 26 the maximum difference and best p-value between the PBO+MTX vs ADA+MTX arms was achieved between ACR70-80 (fig 1B). In pts from DE019 (established RA), ACR35 had the best discriminatory ability and p-value, both at Wks 24 and 52, when comparing PBO+MTX [MTX-continued in MTX inadequate responders (MTX-IR)] vs ADA+MTX (fig 1C). Similarly, in established RA pts from ARMADA, for PBO+MTX vs ADA+MTX at Wk 24, smaller ACR cut-offs were more discriminatory and ACR 30 had the best p-value (fig 1D).
Conclusion: The ACR cut-off score with the best discriminatory ability differed in these 2 populations; In early RA higher ACR cutoffs were more discriminatory, while in established RA, lower ACR cutoffs were better. This may be due to the early RA CTs having active comparator arms with newly introduced MTX, while the established RA CTs control arms had PBO on background MTX in MTX-IR pts. Further analysis is needed to determine if an ACR response other than ACR20, should be used in CTs with a newly introduced active comparator. In addition, the optimal ACR cutoff may differ according to the population studied (early vs. established RA). References
1. Felson et al. 1998. Arth & Rheum;41:1564
2. Breedveld et al. 2006. Arth & Rheum;54:26
3. Smolen et al. 2014. Lancet;383:321
4. Keystone et al. 2004. Arth & Rheum;5:1400
5. Weinblatt et al 2003. Arth & Rheum;48:35
To cite this abstract in AMA style:
Smolen J, Fleischmann R, Aletaha D, Li Y, Florentinus S, Lagunes Galindo I. The Identification of an ACR Score with the Optimal Discriminatory Ability Between Treatments in Patients with Early and Established Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/the-identification-of-an-acr-score-with-the-optimal-discriminatory-ability-between-treatments-in-patients-with-early-and-established-rheumatoid-arthritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-identification-of-an-acr-score-with-the-optimal-discriminatory-ability-between-treatments-in-patients-with-early-and-established-rheumatoid-arthritis/