Session Information
Date: Monday, October 27, 2025
Session Type: Abstract Session
Session Time: 3:00PM-3:15PM
Background/Purpose: Cardiovascular disease is the leading cause of death in systemic lupus erythematosus (SLE).1 Whilst histopathology remains the gold standard for establishing the pathogenesis of cardiac disease, endomyocardial biopsy is invasive and subject to sampling error. We aimed to examine the frequency of cardiovascular disease in SLE compared with the general population, and associations of specific findings with patient outcomes.
Methods: A case-control study was performed using data from the Australian National Coronial Information System, a database of deaths referred for forensic investigation. SLE cases were identified via keyword/ICD-10 code search. Age- and sex-matched controls were selected from victims of motor vehicle accidents. Demographic data and autopsy findings (macroscopic and histopathological) were extracted. Cardiomegaly was defined as heart weight >95th centile for body weight/sex. Odds ratios (OR) were calculated with 95% confidence intervals (CI).
Results: 123 SLE cases and 123 controls were included. Both groups were predominantly female (85%) and of similar age (median SLE 53 (IQR 40-65) years vs. control 54 (41-65) years, p=0.90).After adjusting for age and sex, myocardial fibrosis (OR 3.4, 95%CI 1.8-6.5, p< 0.01), myocardial inflammatory infiltrates (OR 15.5, 95%CI 3.5-68.5, p< 0.01) and pericardial abnormalities (OR 8.9, 95%CI 3.7-21.3, p< 0.01) were significantly more common in SLE (Figure 1). SLE cases were 6.2-times more likely to have cardiomegaly (95% CI 3.2-12.1, p< 0.01). Moderate-to-severe epicardial coronary artery disease (CAD; OR 2.8, 95% CI 1.5-5.2, p< 0.01), myocardial infarction (OR 5.5, 95% CI 1.8-16.7, p< 0.01) and abnormalities of the small intramural coronary vessels (OR 9.6, 95% CI 2.2-42.4, p< 0.01) were more common in SLE after age and sex adjustment. These associations persisted after adjustment for age, sex and moderate to severe CAD (cardiomegaly OR 4.9, 95% CI 2.5-9.7, p< 0.01; myocardial fibrosis OR 3.4, 95%CI 1.8-6.5, p< 0.01; myocyte hypertrophy OR 8.2, 95%CI 2.7-24.8, p< 0.01; small intramural coronary vessel abnormalities OR 9.9, 95%CI 2.2-45.0, p< 0.01). Coronary vasculitis was exclusively identified in 8% of SLE cases. Valvular pathology was more common in SLE (OR 4.9, 95% CI 2.2-10.8, p< 0.01), with vegetations observed in 6% of cases. Cardiovascular death was more common in SLE cases with myocardial fibrosis (OR 2.6, 95% CI 1.1-5.9, p=0.02), moderate-to-severe CAD (OR 4.0, 95% CI 1.8-9.2, p< 0.01) and cardiomegaly (OR 3.6, 95% CI 1.6-7.9, p< 0.01), after adjusting for age and sex (Table 1). Sudden cardiac death was more common in those with cardiomegaly (OR 3.4, 95% CI 1.5-7.5, p< 0.01) and moderate-to-severe CAD (OR 2.5, 95%CI 1.1-5.7, p=0.03), after age and sex adjustment.
Conclusion: SLE is associated with a significant excess of atherosclerotic vascular, inflammatory and fibrotic cardiac lesions. These data highlight the scope of cardiovascular abnormalities occurring in SLE, and their association with cardiovascular causes of death.References1. Taylor T, Anastasiou C, Ja C, et al. Causes of Death Among Individuals With Systemic Lupus Erythematosus by Race and Ethnicity: A Population-Based Study. Arthritis Care Res (Hoboken) 2023; 75(1): 61-8.
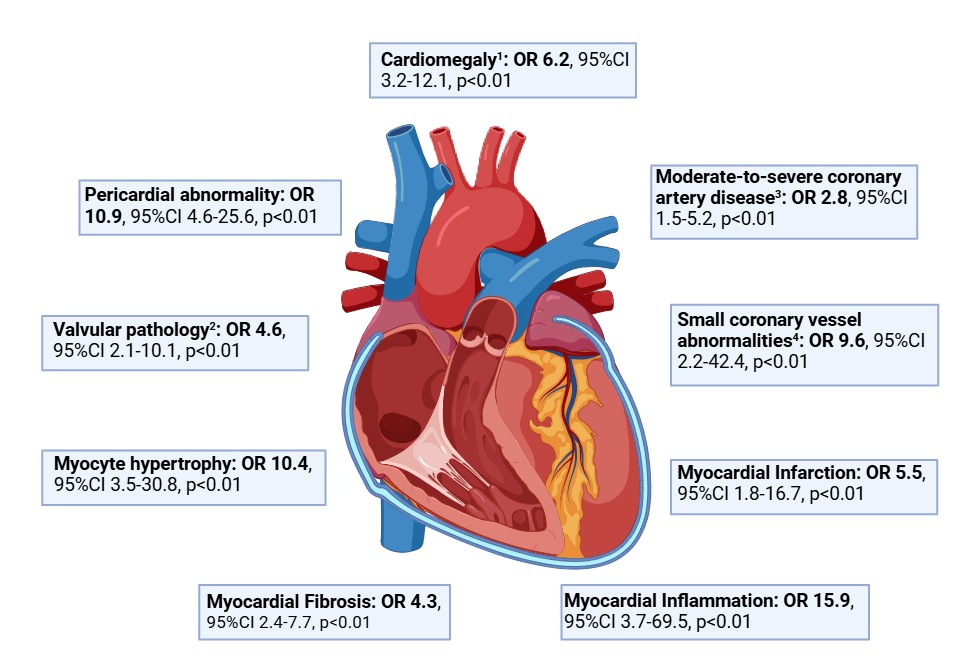 Figure 1: Odds of cardiovascular disease in SLE compared to controls using logistic regression, adjusted for age and sex.
Figure 1: Odds of cardiovascular disease in SLE compared to controls using logistic regression, adjusted for age and sex.
Abbreviations: CI (confidence interval), OR (odds ratio), SLE (systemic lupus erythematosus). 1Cardiomegaly defined as heart weight >95th centile for body weight. 2Valvular pathology defined as at least moderate aortic stenosis, aortic regurgitation, mitral stenosis or mitral regurgitation. 3Coronary artery disease defined as moderate to severe when stenosis >50% vessel occlusion, or qualitative description of “moderate”, “severe” or “critical”. 4Small vessel coronary abnormalities defined as thickening, vasculitis or other abnormality within the small intramural coronary arteries.
.jpg) Table 1: Logistic regression analysis describing the association between cardiovascular abnormalities and both any cardiovascular death and sudden cardiac death in SLE cases only, adjusted for age and sex.
Table 1: Logistic regression analysis describing the association between cardiovascular abnormalities and both any cardiovascular death and sudden cardiac death in SLE cases only, adjusted for age and sex.
Abbreviations: CI (confidence interval), OR (odds ratio), SLE (systemic lupus erythematosus). 1Cardiomegaly defined as heart weight >95th centile for body weight. 2Coronary artery disease defined as moderate to severe when stenosis >50% vessel occlusion, or qualitative description of “moderate”, “severe” or “critical”. 3Valvular pathology defined as at least moderate aortic stenosis, aortic regurgitation, mitral stenosis or mitral regurgitation.
To cite this abstract in AMA style:
Fairley J, Ross L, Paratz E, McKelvie P, Daneshvar S, Oon S, Hansen D, Stevens W, La Gerche A, Nikpour M. The frequency and impact of cardiovascular disease in systemic lupus erythematosus: a Nationwide, matched case-control study. [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/the-frequency-and-impact-of-cardiovascular-disease-in-systemic-lupus-erythematosus-a-nationwide-matched-case-control-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-frequency-and-impact-of-cardiovascular-disease-in-systemic-lupus-erythematosus-a-nationwide-matched-case-control-study/