Session Information
Date: Sunday, October 21, 2018
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: In a Ph2 study, GUS was shown to be safe&effective in pts w/active PsA. We evaluated effect of GUS on dactylitis in subset of pts w/dactylitis at baseline (BL) from Ph2 GUS PsA study.
Methods: Pts w/active PsA & ≥3% BSA of plaque PsO, despite current or previous treatment, were randomized 2:1 to 100mg SC GUS at wks0,4 then q8w or PBO during a 24wk double-blind treatment (tx) period. At wk16, pts w/<5% improvement in swollen&tender joint counts(SJC/TJC) early escaped(EE). At wk24, PBO group(grp) crossed over to GUS (wks24, 28→ q8w)(PBO→GUS) & GUS grp continued GUS (GUS→GUS)) thru wk44. Dactylitis was assessed by scoring each digit from 0-3(0=absent,1=mild,2=mod, 3=sev), for combined score of 0-60. Sensitivity analysis of change from BL thru wk24 in dactylitic digits was performed(combined score 20). Dactylitis scores during 24wk double-blind tx was analyzed using LOCF imputation for missing data & EE. Dactylitis after wk24 was evaluated using observed data.
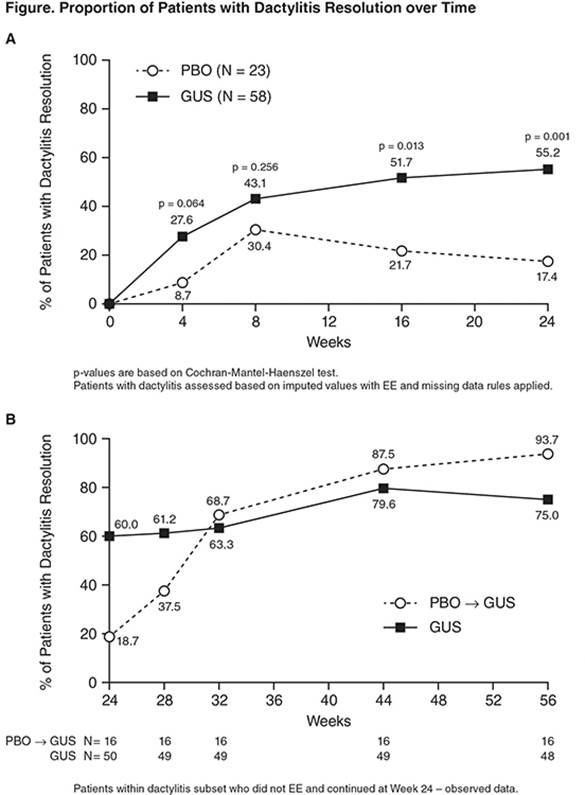
Results: Of 149 pts,81 presented w/dactylitis at BL(PBO N=23,mean[SD]=3.9[3.01];GUS N=58, mean[SD]=6.5[6.15]) & 66 continued to active tx period(PBO→GUS N=16;GUS→GUS N=50).The dactylitis subset was similar to overall population in BL characteristics except for higher median values for # of SJC, # of TJC,&CRP. At wks16&24, GUS grp had significantly greater reduction in dactylitis score(wk24 mean[SD] change from BL,PBO:-0.4[6.06];GUS:-3.8[4.93];p=0.006)&a greater % of pts w/dactylitis resolution vs PBO grp(Figure). Consistent results were obtained w/# digits w/dactylitis(wk24 mean[SD] change from BL, PBO:-0.2[3.04];GUS:-2.1[2.21];p=0.003). Improvement in dactylitis seen at wk24 was maintained in GUS→GUS grp(wk56:mean[SD] change from BL=-5.5[4.84],75% of pts w/resolution)& the values for the PBO→GUS grp(wk56:mean[SD]change from BL=-4.4[3.50],93.7% of pts w/resolution)approached those of GUS→GUS grp. Improvement in dactylitis was greater in ACR20/ACR50 responders vs non-responders in GUS-txd pts(Table)&was significantly correlated with improvement in TJC(R=0.38,p=0.004),SJC(R=0.50,p<0.0001),&HAQ-DI score(R=0.33,p=0.013).
Conclusion: GUS is efficacious in resolving symptoms of dactylitis in pts w/active PsA. This effect on dactylitis is correlated with improvement in joint symptoms & physical function.

|
Table 1. Change in Dactylitis Score in ACR20/50 and PASI75 Responders and Non-responders |
|||
|
Mean (SD) change from BL in Dactylitis Score at Wk24 |
|||
|
Non-responders |
Responders |
p-value |
|
|
ACR 20 |
-1.76(7.595), n=21 |
-4.94(4.666), n=36 |
0.044 |
|
ACR 50 |
-2.44(6.213), n=36 |
-6.05(5.133), n=21 |
0.027 |
|
PASI 75 |
-4.00(2.858), n=13 |
-3.70(6.736), n=44 |
0.924 |
To cite this abstract in AMA style:
Gladman DD, Boehncke WH, Gottlieb AB, Helliwell P, Nash P, Xu XL, Xu S, Wang Y, Hsia EC, Karyekar CS, Deodhar AA. The Effect of Guselkumab on Dactylitis: Results from a Phase 2 Study in Patients with Active Psoriatic Arthritis [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/the-effect-of-guselkumab-on-dactylitis-results-from-a-phase-2-study-in-patients-with-active-psoriatic-arthritis/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-effect-of-guselkumab-on-dactylitis-results-from-a-phase-2-study-in-patients-with-active-psoriatic-arthritis/