Session Information
Date: Sunday, October 26, 2025
Title: Abstracts: Orthopedics, Low Back Pain, & Rehabilitation (0783–0788)
Session Type: Abstract Session
Session Time: 2:00PM-2:15PM
Background/Purpose: Based on several RCTs comparing outcomes of arthroscopic partial meniscectomy (APM) to non-operative management in persons with meniscal tears and OA, physical therapy (PT) is now considered the first line treatment. The TeMPO (Treatment of Meniscal Tears in Patients with Osteoarthritis) trial established that an in-clinic PT program with home exercise component led to a small incremental pain reduction at 6 and 12 months compared to home exercise alone. We sought to determine the cost-effectiveness of PT with home exercise compared to home exercise alone using data from the TeMPO trial.
Methods: We used the Osteoarthritis Policy (OAPol) Model, a widely published and validated microsimulation of knee OA, to compare two strategies: 1) home-based exercise (HE) vs. 2) Physical Therapy focused on strengthening (PT) plus HE. The 5-year outcomes included quality-adjusted life expectancy and costs. Patients in both strategies could subsequently transition to APM, corticosteroid injections, opioids, total knee replacement (TKR), and revision TKR, if the initial treatment did not lead to meaningful pain relief. We modeled pain trajectories at baseline, 3, 6, and 12 months based on strategy-specific data from TeMPO (HE: 47, 29, 28 and 24 vs. PT: 45, 26, 22, 20 points, on a scale 0-100, 0 being no pain). We also derived APM, 1-year TKR, and opioid utilization from the overall TeMPO cohort, due to negligible observed difference across arms (11% had APM, 1% had TKR, 2% used opioids). We derived 5-year TKR utilization from the non-operative arm in the MeTeOR trial, which followed patients with meniscal tear and concomitant OA over 5 years (TKR use ~ 4% over 5 years). The cost of the home exercise regimen included analgesic medications, home exercise guides and materials ($213). In addition to these costs, the cost of the PT regimen included exercise bands, pamphlets, reminder texts, and evaluation and treatment visits ($1,540). We conducted the analysis for a cohort with mean age 59, KOOS pain 46 (0-100, 100 worst), and mean BMI 30 kg/m2. We calculated incremental cost-effectiveness ratios (ICERs) as the difference in lifetime costs (2024 USD) divided by the difference in quality-adjusted life years (QALYs) between two strategies. We used a health care perspective and discounted clinical benefits and costs at 3% annually. We conducted sensitivity analyses to determine how uncertainty in input parameters might affect our findings.
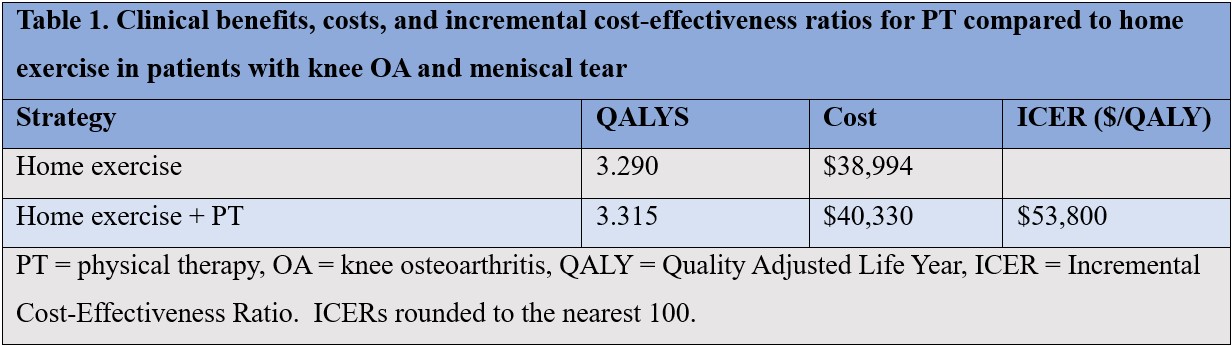
Results: Adding PT increased the 5-year quality-adjusted life expectancy by 0.03 QALYs at the additional cost of $1,300/person, resulting in an estimated ICER for PT of $53,800/QALY (Table 1). The two parameters with the largest effect on the ICER were the difference in pain efficacy between the two regimens and the starting pain of the cohort. When the difference in pain efficacy decreased by 50%, the ICER for PT increased to $142,500/QALY. If starting pain would be reduced by about 25%, the ICER would increase to $72,700/QALY.
Conclusion: Despite relatively small incremental clinical benefits, physical therapy with the home exercise component could be a cost-effective strategy at any cost-effectiveness threshold exceeding $53,800/QALY.
To cite this abstract in AMA style:
Chin S, Aronson S, Collins J, Selzer F, Yang Y, Bisson L, Chen A, Jones M, Norton C, Smith K, Spindler K, Katz J, Losina E. The Cost-effectiveness of Physical Therapy for Patients with Meniscal Tear and Osteoarthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/the-cost-effectiveness-of-physical-therapy-for-patients-with-meniscal-tear-and-osteoarthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-cost-effectiveness-of-physical-therapy-for-patients-with-meniscal-tear-and-osteoarthritis/