Session Information
Date: Sunday, November 7, 2021
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster II: Manifestations (0855–0896)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Current guidelines recommend use of hydroxychloroquine (HCQ) at doses not exceeding 5mg/kg based solely on the increased risk of retinopathy at higher doses. This recommendation does not consider the impact of HCQ dose in comorbidities, disease activity or outcomes. Both protective and toxic effects of HCQ on cardiovascular health have been reported but how HCQ dose influences this balance is uncertain. We aimed to determine if HCQ dose is associated with all-cause heart failure with reduced ejection fraction (HFrEF), life-threatening arrhythmia or cardiac death in SLE.
Methods: This was a retrospective cohort study of SLE patients followed at a tertiary care center in the Bronx, New York between January 2005 and January 2021. SLE patients on HCQ with at least one echocardiogram were included. HCQ weight-based doses at HCQ start date and through follow up were recorded. The primary outcome was incident all-cause HFrEF, life-threatening arrhythmia or cardiac death. HFrEF was defined as documentation of clinical heart failure and a systolic ejection fraction < 50% on echocardiogram. Arrhythmia was defined as ventricular arrhythmia, sudden cardiac death, or need for implantable cardiac device or pacemaker. We used competing risk regression to study the association of HCQ dose with the composite outcome. Due to a significant interaction between smoking and HCQ exposure, models were stratified by smoking status.
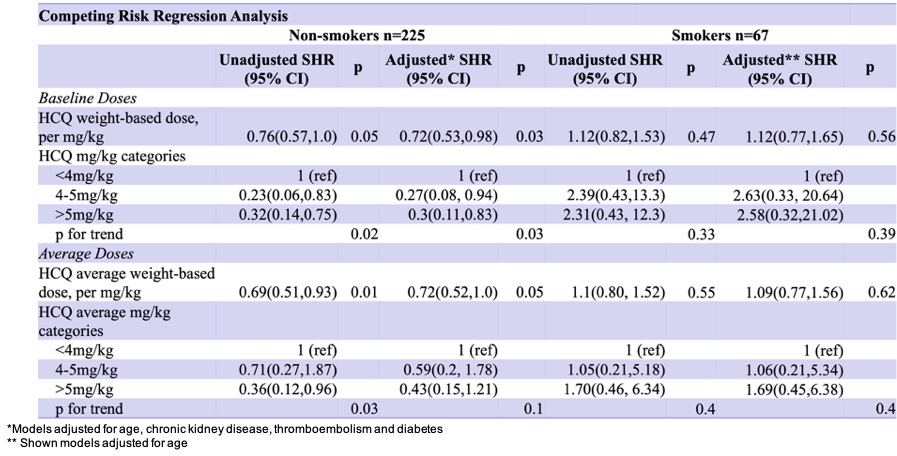
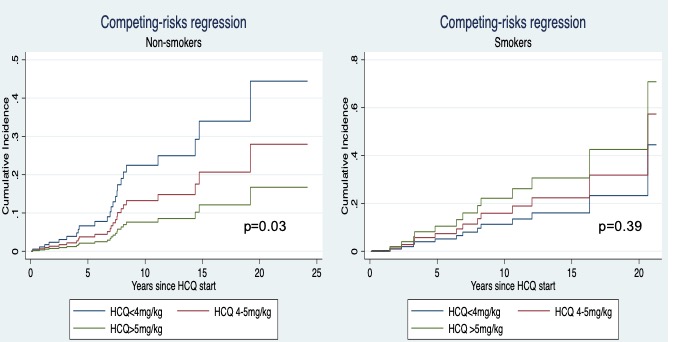
Results: Of 296 patients, 38 (13%) developed the outcome over a median (IQR) follow up time of 7.0 (3.3,11.8) years. Mean age at baseline (HCQ start date) was 33 ± 13.6 years. A total of 267 (90%) were female and 278 (94%) self-identified as Hispanic or Black. At baseline, 97 (33%) had lupus nephritis, 44 (15%) had chronic kidney disease stage 3 or higher, 26 (9%) had a history of thromboembolism or antiphospholipid syndrome, 101 (34%) had hypertension, 68 (23%) were smokers, 11 (4%) had diabetes and 7 (2%) had coronary artery disease. Mean HCQ weight-based dose was 5.2 ± 1.5 mg/kg at baseline and 5.1 ± 1.5 in average through follow up. Median (IQR) HCQ duration and cumulative dose were 6.5 (3.1, 11.3) years and 828 (328, 1467) grams, respectively. In non-smokers (n=225), multivariable analysis adjusted for age, chronic kidney disease, diabetes and thromboembolism showed that the risk of HFrEF or arrhythmia decreased by 28% per mg/kg of baseline HCQ dose, HR 0.72 (95% CI 0.53, 0.98), p=0.03 (Table). The cumulative incidence of the outcome was the lowest at doses >5mg/kg (Figure). Conversely, there was no significant association between higher baseline HCQ doses and the risk for the outcome among smokers (n=67), HR 1.12 (95% CI 0.77, 1.65) per mg/kg, p=0.56.
Conclusion: Higher HCQ doses were associated with a lower risk HFrEF, life-threatening arrhythmia or cardiac death among non-smoker SLE patients and no increased risk among smokers. If confirmed with future studies, these results would support the inclusion of the potential cardiovascular benefits derived from higher HCQ dosing into HCQ dosing risk-benefit considerations, beyond the risk for retinopathy.
References:
Fanouriakis A et al. Ann Rheum Dis. 2019
Marmor MF et al. Ophthalmology. 2016
To cite this abstract in AMA style:
Londono Jimenez A, Mustehsan M, Valle A, Law J, Wang S, Salgado Guerrero M, Briceno D, Broder A. The Association of Hydroxychloroquine Dosing with Adverse Cardiovascular Events in Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/the-association-of-hydroxychloroquine-dosing-with-adverse-cardiovascular-events-in-patients-with-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-association-of-hydroxychloroquine-dosing-with-adverse-cardiovascular-events-in-patients-with-systemic-lupus-erythematosus/