Session Information
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Measurement of disease activity is considered a quality measure for management of rheumatoid arthritis (RA) patients. One validated measure of RA disease activity is the Routine Assessment of Patient Index Data 3 (RAPID3) score. We developed a quality improvement project to improve our clinic’s adherence to use of the RAPID3 score in our patients with RA, with the goal of increasing documentation by 25% from baseline.
Methods: In our academic practice, we surveyed providers regarding their preferred disease activity measurement; the RAPID3, already utilized in our clinic, was preferred by the majority of providers. Patient charts were screened for presence or absence of RAPID3 score within providers’ notes. Using Plan-Do-Study-Act (PDSA) methodology, we introduced the following interventions to improve provider documentation: education through Divisional Grand Rounds, direct modification of electronic medical record (EMR) templates, and posted reminders in clinic. Chart review was conducted between interventions and at the conclusion of all interventions. A repeat survey of providers assessed providers’ responses to the interventions and utilization of the RAPID3 in clinical decision making.
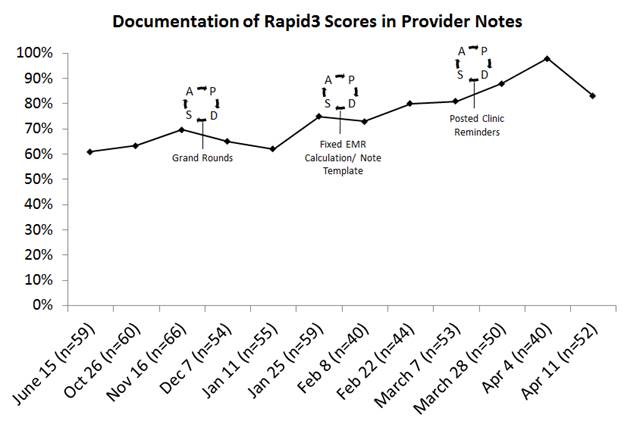
Results: Review of 3054 charts identified 632 patients with RA. At baseline, an average of 65% of provider progress notes documented a RAPID3 score. For the 3 months following the last intervention, the provider documentation rate had increased to an average of 90%, a 38% increase from baseline (see figure). Reasons for missing RAPID3 documentation include incomplete data entry during check-in. Providers noted the most helpful interventions to be changing their note template in the EMR (40%), Grand Rounds discussions (33%), and posted clinic reminders (13%). At the conclusion of the QI initiative, 20% of providers reported using the Rapid3 for clinical decision making in 50-74% of cases, while 53% used the Rapid3 25-49% of the time, and 27% reported using the Rapid3 <25% of the time; no one reported never using the Rapid 3 for clinical decision making, and no one reported using it >75% of the time.
Conclusion: We demonstrated sustained improvement in documentation of RAPID3 scores, increasing documentation rates by 38%. One barrier to successful implementation of this score was correct calculation within the EMR, which was challenging to rectify. Once corrected, documentation of the disease activity measure increased. However, we found that the majority of clinicians reported using the RAPID3 in their medical decision making less than 50% of the time, despite stating a preference for this measure in the practice. With the RAPID3 now incorporated into our practice’s daily use, assessment of overall clinical response rate will be possible along with ongoing efforts to increase utilization of this quality measure for medical decision making to improve quality of patient care in RA.
To cite this abstract in AMA style:
Wells M, Sadun R, Jayasundara M, Holdgate N, Mohammad S, Weiner J, Haroun T, Balevic S, Criscione-Schrieber L, Kaul M. Sustained Improvement in Documentation of Disease Activity Measurement As a Quality Improvement Project at an Academic Rheumatology Clinic [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/sustained-improvement-in-documentation-of-disease-activity-measurement-as-a-quality-improvement-project-at-an-academic-rheumatology-clinic/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sustained-improvement-in-documentation-of-disease-activity-measurement-as-a-quality-improvement-project-at-an-academic-rheumatology-clinic/