Session Information
Date: Sunday, November 7, 2021
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: The primary treatment target for patients with active rheumatoid arthritis (RA) is sustained clinical remission (REM) or low disease activity (LDA).1,2 A greater proportion of patients with RA and inadequate response to methotrexate (MTX) receiving the JAK inhibitor, upadacitinib (UPA), achieved REM/LDA compared with adalimumab (ADA), both with background MTX, through 26 weeks in the phase 3, SELECT-COMPARE trial.3 Here we assessed sustainability of response over 3 years.
Methods: SELECT-COMPARE included a 26-week, double-blind, placebo (PBO)-controlled period, a 48-week, double-blind active comparator-controlled period, and an ongoing long-term extension for up to 10 years. Patients on background MTX received UPA 15 mg once daily, PBO, or ADA 40 mg every other week. Patients who did not achieve at least 20% improvements in tender and swollen joint counts (Weeks 14-22) or LDA (CDAI ≤10 at Week 26) were rescued from UPA to ADA or PBO/ADA to UPA. This post hoc analysis evaluated clinical REM (CDAI ≤2.8; SDAI ≤3.3), LDA (CDAI ≤10; SDAI ≤11), and DAS28(CRP) < 2.6/≤3.2 at first occurrence (prior to treatment switch [rescue]), as well as over 3 years following initial response in patients randomized to UPA or ADA. For those patients who achieved REM/LDA, Kaplan-Meier was used to define the time from when the response was first achieved to the earliest date at which the response was lost at two consecutive visits, discontinuation of study drug, or losing response at the time of rescue. The predictive ability of time to CDAI REM/LDA was assessed using Harrell’s concordance (c)-index (range: 0 [all predictions wrong] to 1.0 [perfect predictive ability]. Non-responder imputation was used for missing data.
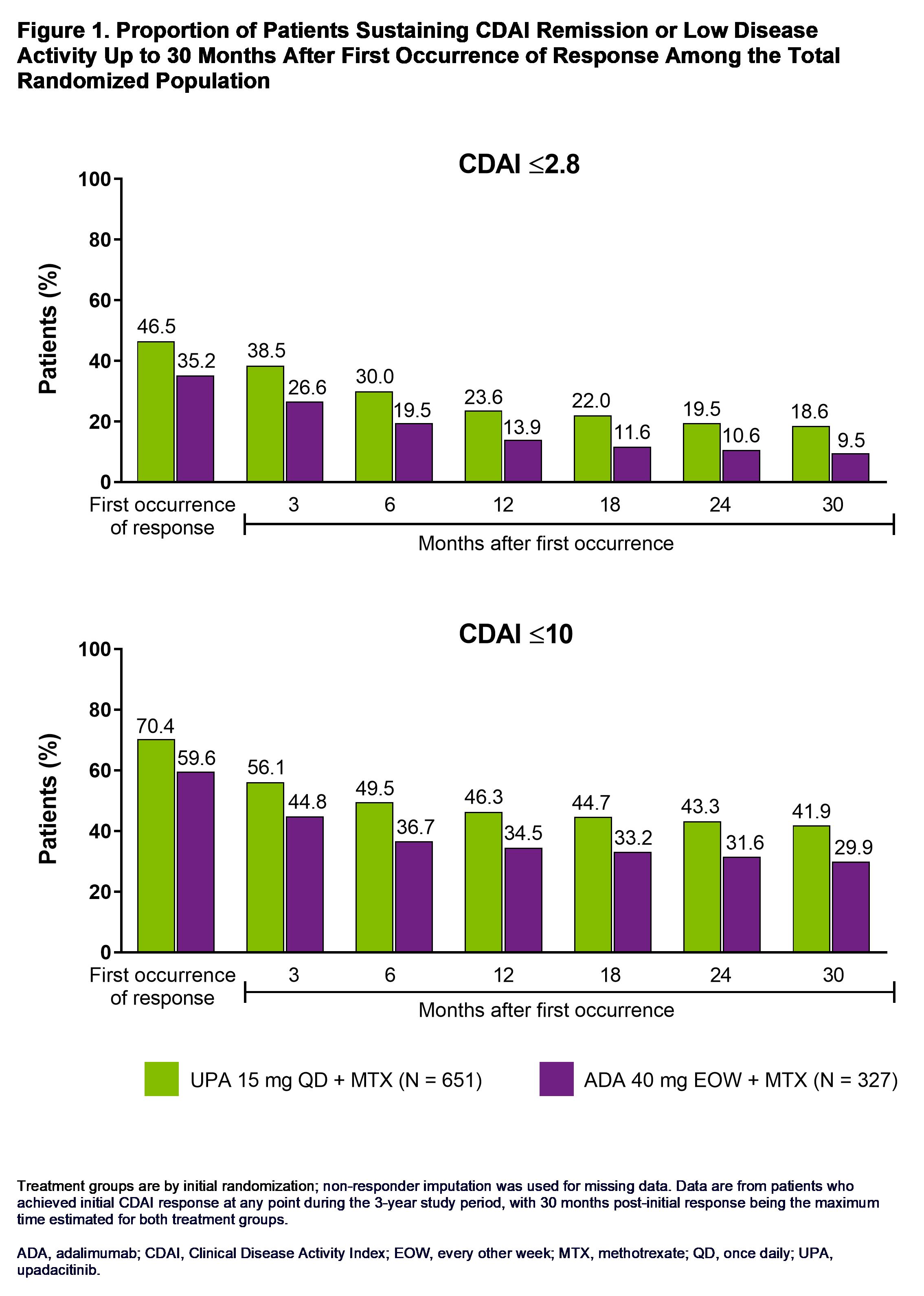
Results: Through 3 years, a significantly higher proportion of patients receiving UPA + MTX vs ADA + MTX achieved CDAI REM (47% vs 35%, P = 0.001) as well as CDAI LDA (70% vs 60%, P = 0.001). At 30 months after first occurrence of response, CDAI REM/LDA was sustained in 19%/42% of patients randomized to UPA and 10%/30% of patients randomized to ADA (Figure 1). Time to initial clinical response did not appear to be predictive of sustained disease control. The c-index for CDAI REM/LDA was 0.50/0.60 on UPA vs 0.49/0.56 on ADA. Through the last follow-up visit, 37%/58% of patients receiving UPA and 27%/48% on ADA remained in CDAI REM/LDA, respectively (Figure 2). Of patients who lost CDAI REM, 68% on UPA and 55% on ADA remained in LDA. Additionally, roughly similar proportions on UPA and ADA recaptured CDAI REM/LDA (UPA, 40%/17%; ADA, 48%/19%). Similar results were observed for REM/LDA based on SDAI and for DAS28(CRP) < 2.6/≤3.2.
Conclusion: Among patients with inadequate response to MTX, a higher proportion receiving UPA + MTX achieved remission or LDA across disease activity measures vs ADA + MTX. UPA-treated patients demonstrated a consistently higher sustained response rate over 3 years compared to those receiving ADA. Furthermore, significant proportions of patients who lost response on either UPA or ADA were able to recapture remission or LDA.
References:
1. Smolen et al. Ann Rheum Dis 2020;79:685–99.
2. Singh et al. Arthritis Rheumatol 2016;68:1–26.
3. Fleischmann et al. Arthritis Rheumatol 2019;71:1788–1800.

To cite this abstract in AMA style:
Nash P, Kavanaugh A, Buch M, Combe B, Bessette L, Song I, Shaw T, Song Y, Suboticki J, Fleischmann R. Sustainability of Response Between Upadacitinib and Adalimumab in Patients with Rheumatoid Arthritis: Results Through 3 Years from the SELECT-COMPARE Trial [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/sustainability-of-response-between-upadacitinib-and-adalimumab-in-patients-with-rheumatoid-arthritis-results-through-3-years-from-the-select-compare-trial/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sustainability-of-response-between-upadacitinib-and-adalimumab-in-patients-with-rheumatoid-arthritis-results-through-3-years-from-the-select-compare-trial/