Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Rheumatoid arthritis (RA) is associated with increased risk of cardiovascular disease (CVD), venous thromboembolism (VTE), and mortality. Many patients with RA underwent knee and hip replacement surgeries, i.e., knee arthroplasty and hip arthroplasty. The primary role of knee arthroplasty and hip arthroplasty is to remove the structural abnormality, leading to significant improvements in pain and function. However, the aforementioned improvements may not translate into a lower risk of all-cause mortality, one of the most important indicators for the net risk-benefit effect of any clinical treatment regimen, among patients with RA. Considering physical inactivity and use of non-steroidal anti-inflammatory drugs (NSAIDs) are major risk factors for CVD, one would anticipate that there is a potential cardioprotective advantage coupled with knee arthroplasty and hip arthroplasty as they enhance the capacity for physical activity and reduced usage of analgesics (e.g., NSAIDs). Nevertheless, the impact of these surgeries on CVD risk among patients with RA also needs to be yet confirmed. We aimed to examine the relation of knee or hip arthroplasty to the risk of all-cause mortality, CVD and VTE among patients with RA.
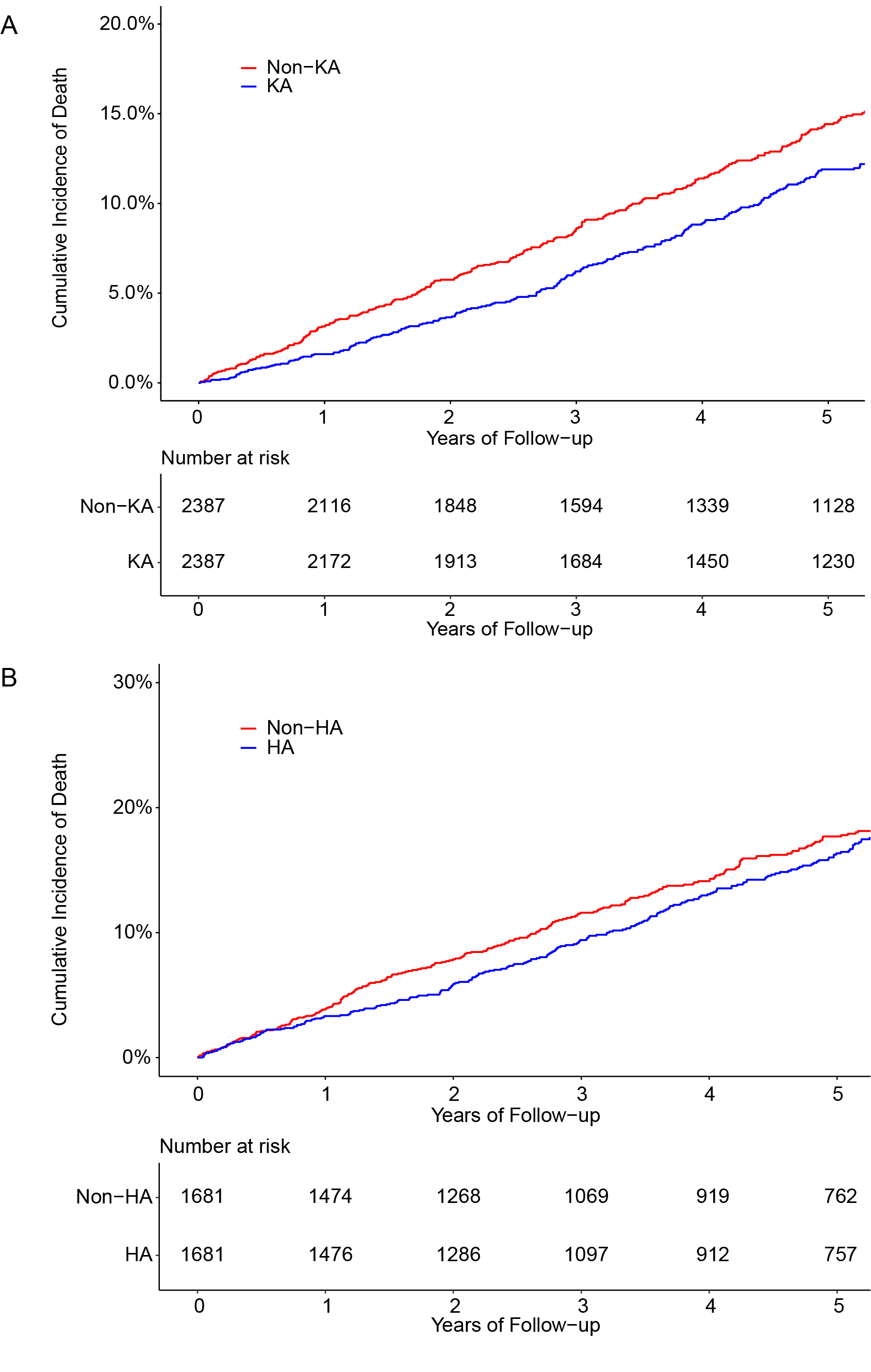
Methods: We included patients with RA (ages≥20 years) from the IQVIA Medical Research Data primary care database in the United Kingdom. The primary outcome was all-cause mortality. The secondary outcomes included CVD and VTE. We conducted propensity score-matched cohort studies to compare the risks of each outcome between subjects with knee arthroplasty (n=2,387) and hip arthroplasty (n=1,681), and those without knee arthroplasty (n=2,387) or hip arthroplasty (n=1,681), respectively.
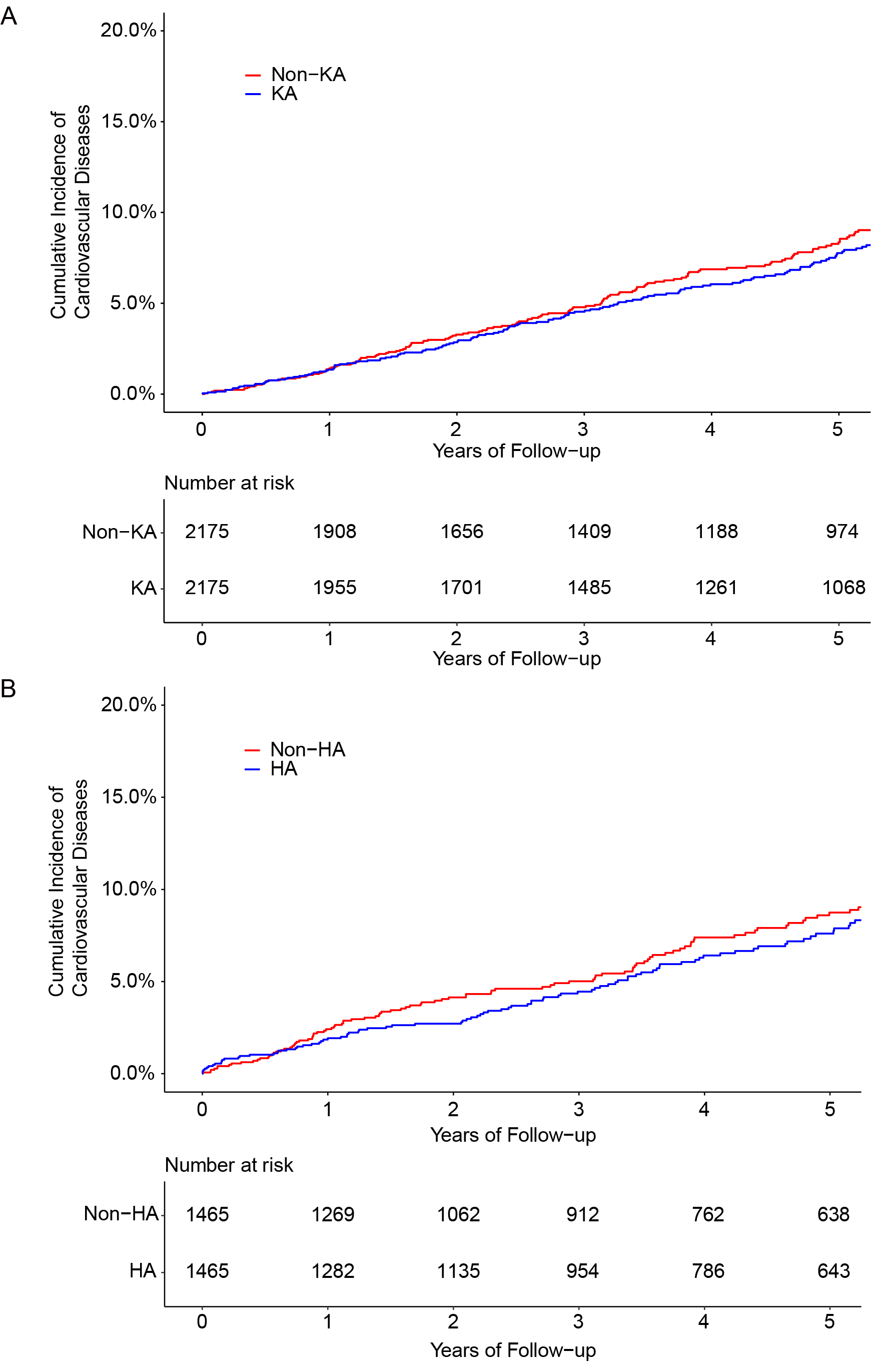
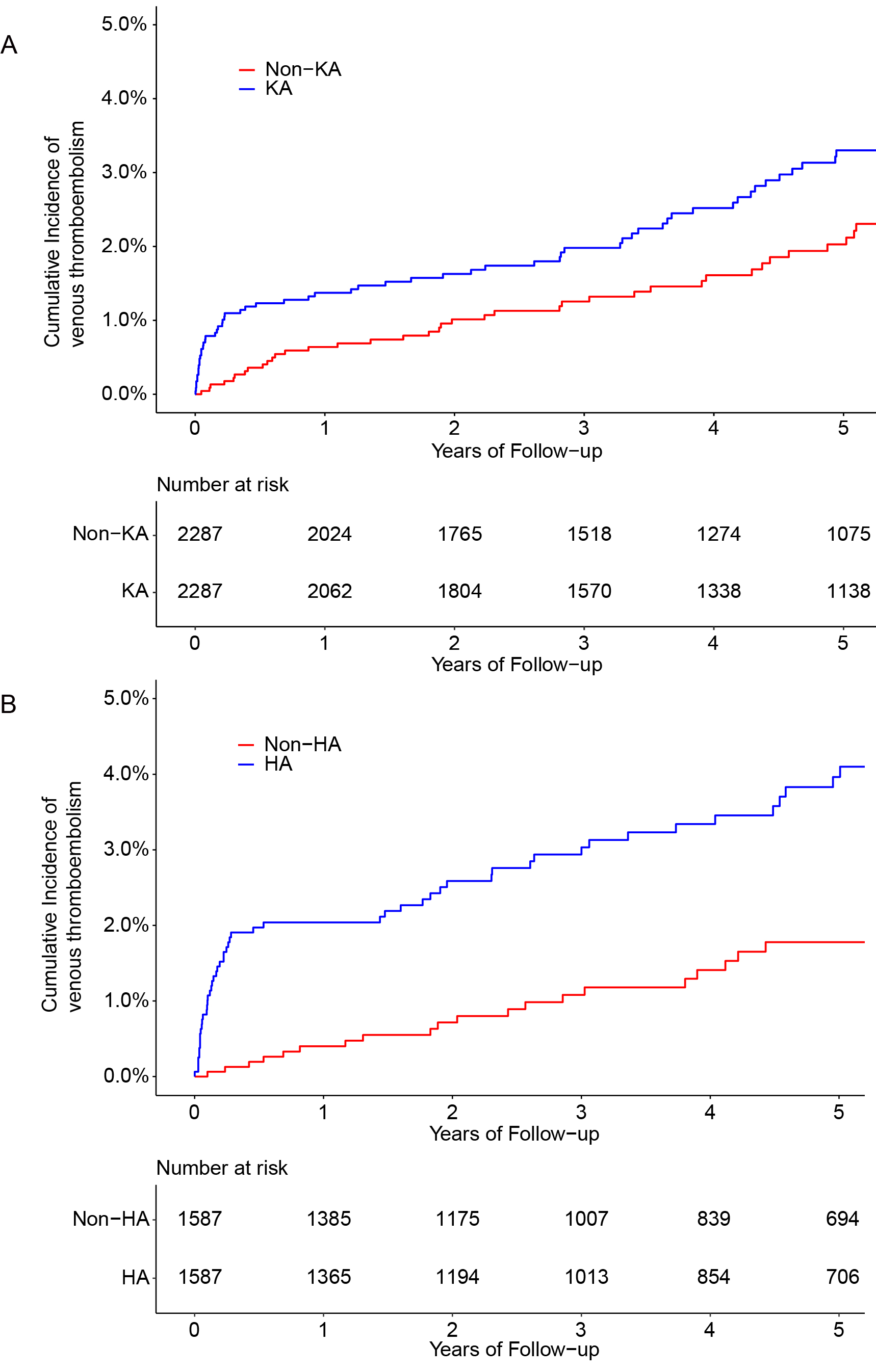
Results: Subjects with knee arthroplasty had 23% lower risk of mortality than those without knee arthroplasty (HR: 0.77, 95%CI: 0.65-0.90) (Figure 1A). Similarly, a lower, albeit non-statistically significant, mortality rate was observed among subjects with hip arthroplasty than those without arthroplasty (HR: 0.87, 95%CI: 0.73-1.04) (Figure 1B). Compared with those without arthroplasty, subjects with knee or hip arthroplasty had a lower, albeit non-statistically significant, risk of CVD. The corresponding HRs were 0.86 (95%CI: 0.73-1.01) and 0.84 (95%CI: 0.69-1.02), respectively (Figure 2). Both subjects with knee or hip arthroplasty showed a higher risk of VTE than their counterparts (HR for knee arthroplasty: 1.63 (95%CI: 1.23-2.17); HR for hip arthroplasty: 2.19 (95%CI: 1.54-3.11) (Figure 3). The associations of knee and hip arthroplasty with the risks of mortality, CVD and VTE were generally consistent across strata of age and sex.
Conclusion: Our population-based cohort study provides the first evidence that knee and hip arthroplasty were associated with lower risks of mortality and CVD but increased risk of VTE among patients with RA.
To cite this abstract in AMA style:
Deng X, Zhang Y, Wang Y, Lu N, Xie D, Lyu H, Wei J, Zeng C, Lei G, Li H. Survival Benefits of Knee and Hip Arthroplasty in Patients with Rheumatoid Arthritis: A General Population-based Cohort Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/survival-benefits-of-knee-and-hip-arthroplasty-in-patients-with-rheumatoid-arthritis-a-general-population-based-cohort-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/survival-benefits-of-knee-and-hip-arthroplasty-in-patients-with-rheumatoid-arthritis-a-general-population-based-cohort-study/