Session Information
Date: Sunday, November 17, 2024
Title: Orthopedics, Low Back Pain, & Rehabilitation – ACR/ARP Poster
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Prior research has shown that compared to individual PT, group-based physical therapy (Group PT) yields equivalent or greater improvement in outcomes for patients with knee osteoarthritis (OA), and it is a more efficient delivery model. Little is known about optimal strategies for supporting implementation of new clinical programs like Group PT into outpatient rehabilitation settings. We conducted a randomized hybrid effectiveness-implementation trial comparing two implementation approaches to support spread of Group PT. We describe implementation outcomes for the two study arms.
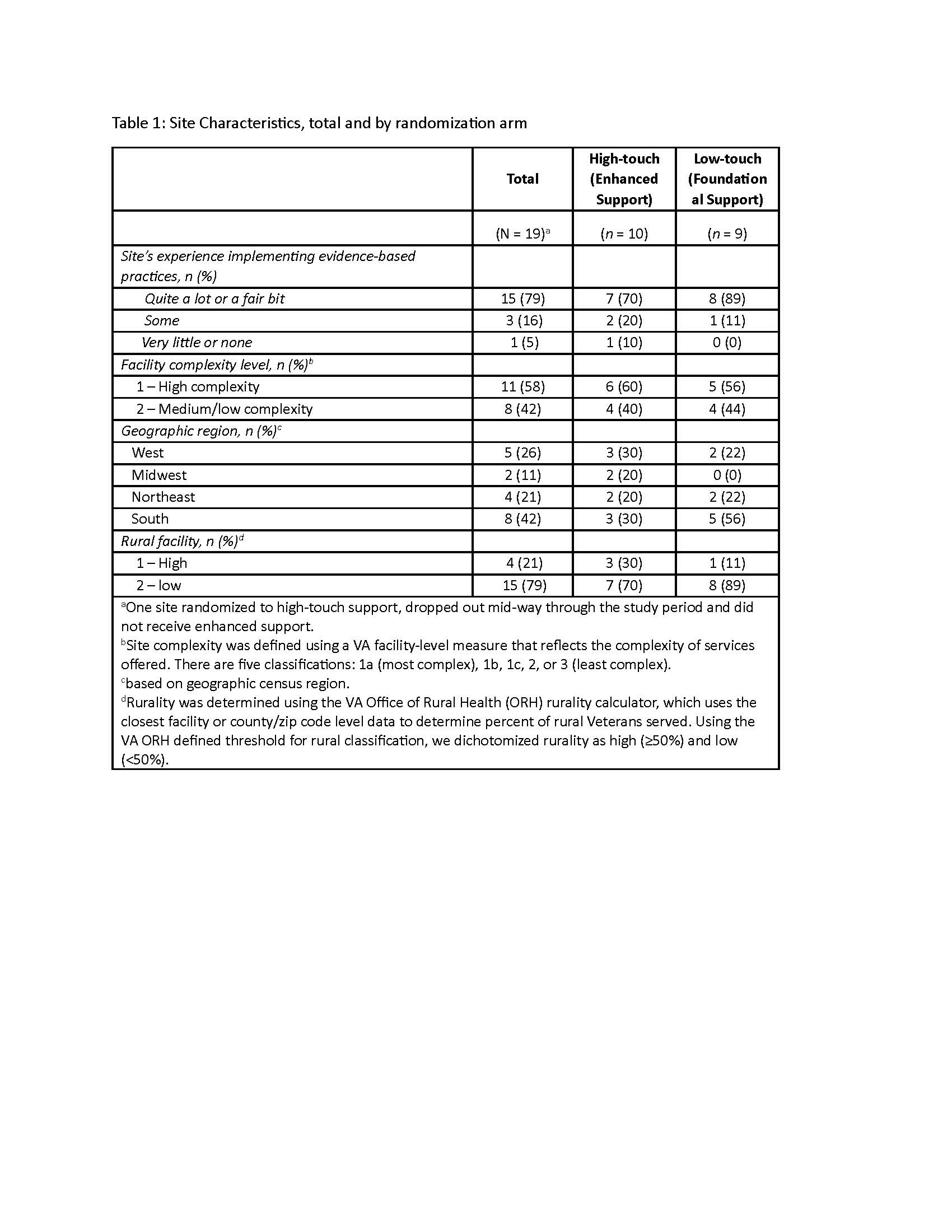
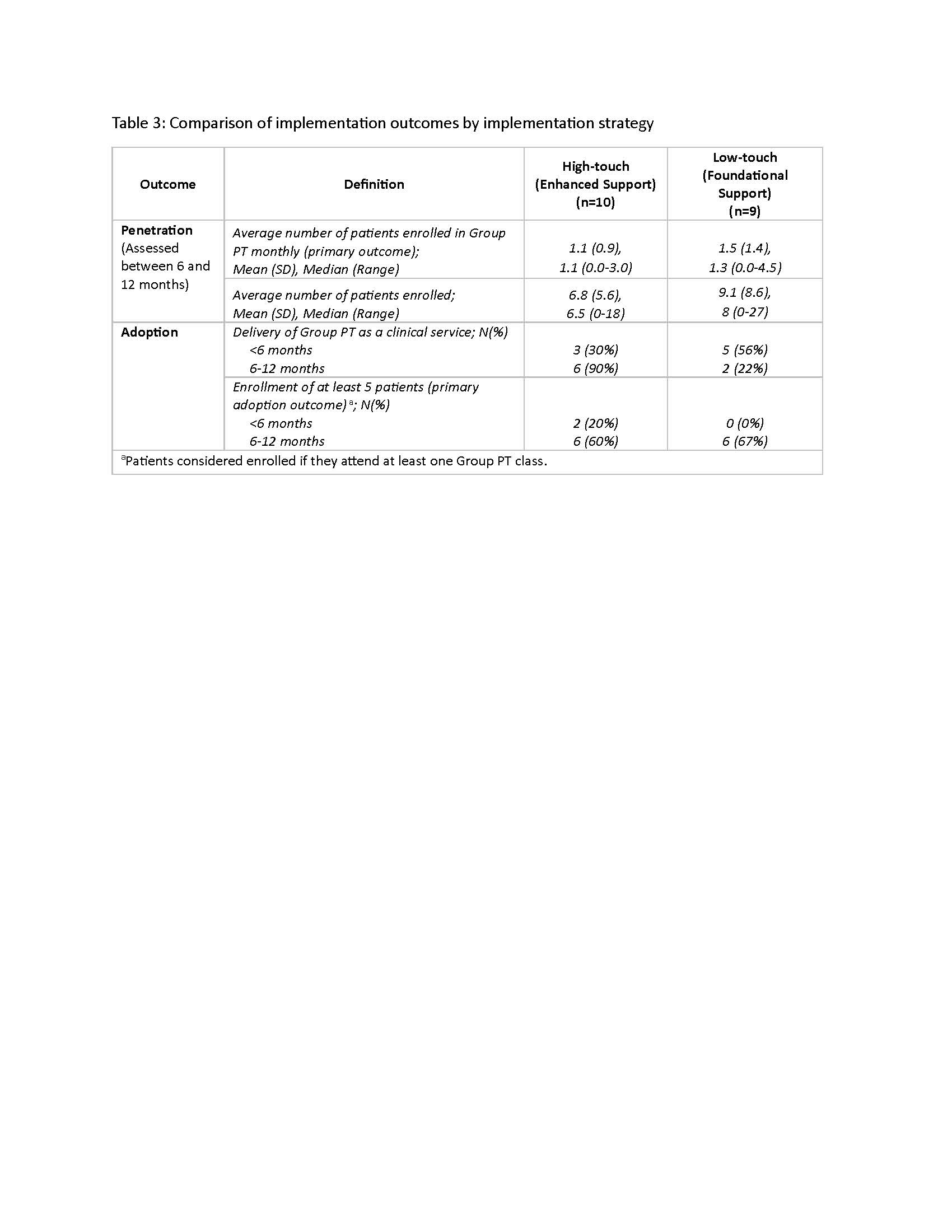
Methods: Nineteen VA medical centers (VAMCs) were enrolled across 3 cohorts (June 2021-February 2023). Sites were randomized to receive one of two implementation support approaches delivered over a 12-month period. The first approach was foundational, low-touch support, consisting of self-guided tools and monthly group / learning collaborative “office hour” calls. The second approach was enhanced support, consisting of foundational support plus the addition of high-touch support (e.g., 1:1 coaching calls delivered by an external facilitator) for sites that did not meet program benchmarks for adoption or sustainment at 6 and 9 months, respectively. Implementation outcomes included penetration (primary outcome) and adoption (see Table 3 for definitions), focused on the time period between 6 and 12 months after the beginning of foundational support (as high-touch sites could only receive additional support after 6 months). Data were collected using the VA’s electronic health record. Descriptive statistics were computed for implementation outcomes by study arm.
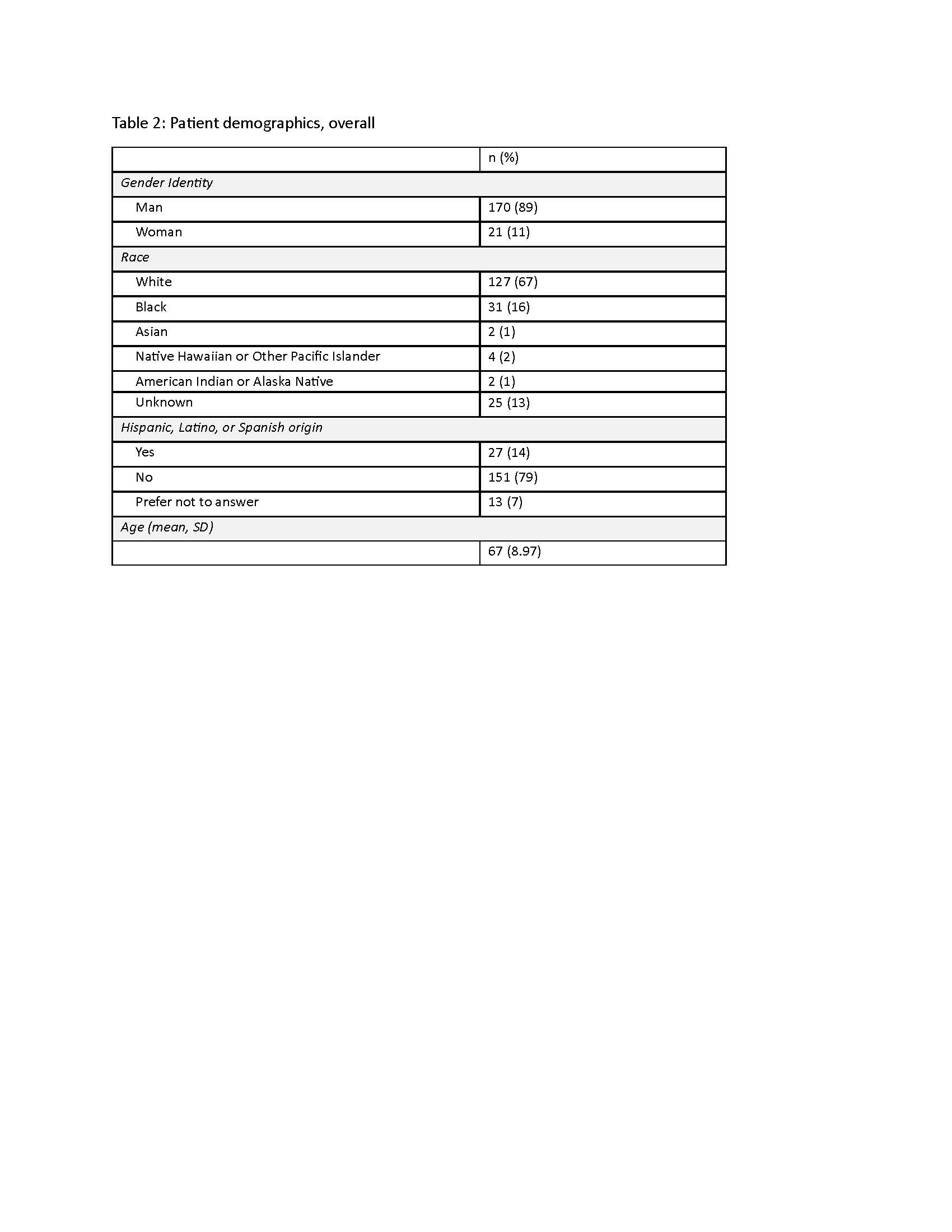
Results: Table 1 shows characteristics of low-touch and high-touch sites, and Table 2 shows characteristics of patients enrolled in Group PT. Sixteen of 19 sites successfully delivered a Group PT program during the study period; of these, 10 offered in-person classes while 6 offered virtual classes. All high-touch sites received additional support, as they did not meet benchmarks for either adoption (6 sites) or sustainment (3 sites). Table 3 shows implementation outcomes by study arm. Observed penetration during the 6-12 month time period was slightly greater for low-touch sites compared to high-touch sites (mean number of enrolled patients: 9.1 and 6.8, respectively). During the 6-12 month time period, 67% of low-touch and 60% of high-touch sites met the primary adoption outcome benchmark; 2 additional high-touch sites met the primary adoption benchmark prior to 6 months.
Conclusion: The high-touch implementation approach does not appear to out-perform the low-touch approach based on the observed data. These results are important since a low-touch implementation approach is feasible and more cost efficient to apply at scale. The rate of Group PT adoption was high, though penetration was modest and varied considerably, illustrating the challenge of fostering referrals at some sites.
To cite this abstract in AMA style:
Allen K, Webb S, Anderson L, Abbate l, Ballengee L, Coffman C, Drake C, Cummin G, Hoenig H, Hughes J, Sperber N, Tucker M, Webster A, Zullig L, Van Houtven C, Hastings S. Supporting Implementation of Group Physical Therapy for Knee Osteoarthritis: Results of a Multisite Implementation Trial [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/supporting-implementation-of-group-physical-therapy-for-knee-osteoarthritis-results-of-a-multisite-implementation-trial/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/supporting-implementation-of-group-physical-therapy-for-knee-osteoarthritis-results-of-a-multisite-implementation-trial/