Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Many factors contribute to long wait times for new patient rheumatology visits including the increasing number of rheumatology referrals and new patient visits. Through a separate retrospective analysis, we found that many new patients (32%) in our rheumatology clinics likely did not need to see rheumatology and could have been evaluated via e-Consult (72%). In addition, with the expansion and acceptance of telemedicine, we postulated a new patient video triage program could facilitate appropriate care while also avoiding unnecessary in-person rheumatology appointments.
Methods: New patients scheduling a rheumatology appointment from December 2022 through May 2023 were offered a video triage appointment option with a rheumatology provider at our tertiary academic medical center. Patients were advised this appointment would determine whether they would need subsequent evaluation or follow-up with rheumatology. If appropriate after evaluation, they were scheduled for an in-person appointment (average of 2 weeks later). Subsequently, a chart review was completed to validate our primary outcome of interest: need of in-person rheumatology follow-up. We also compared the 2 groups of patients: those that needed in-person rheumatology follow up vs. those that did not need follow-up to evaluate for differences in terms of visit reason and referral source. Lastly, we measured the difference in median wait times for video vs in-person new appointments.
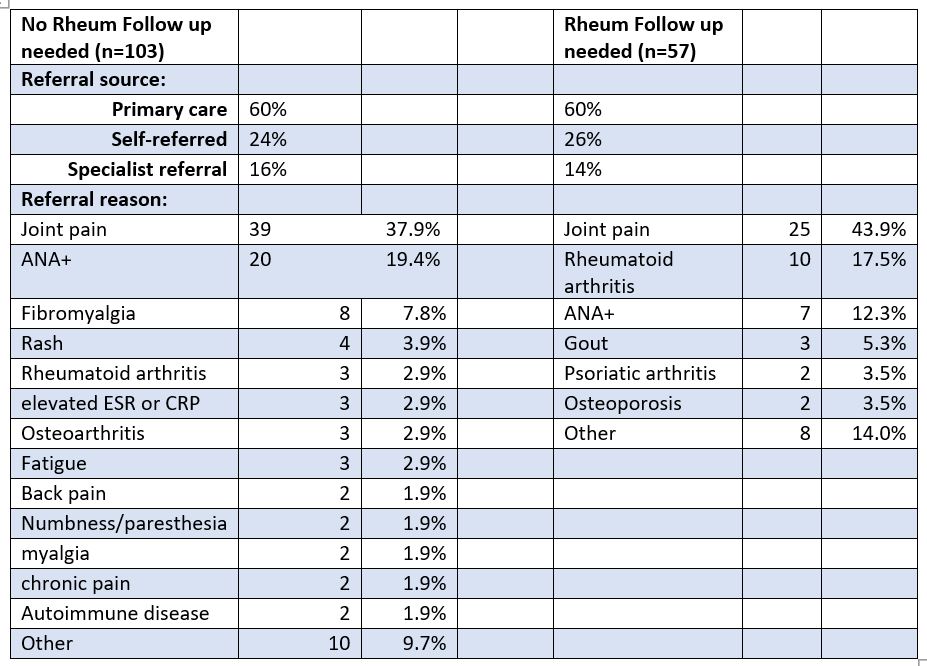
Results: A total of 225 patients were included in the rheumatology new patient video triage program. Of these, 103 (46%) patients were found to not require an in-person rheumatology follow up and were referred back to their primary care provider or another specialty for follow-up. Only 57 (25%) patients required a subsequent in-person rheumatology follow up. A total of 26 (12%) patients did not show to or cancelled their appointments. 14 (6%) patients did not complete follow-up testing after the video appointment. The remaining 25 patients are currently being assessed to determine if ongoing rheumatology care is needed. Referral sources were similar between patients who required rheumatology follow-up and those who did not (Table 1). Reasons for initial visit are shown in Table 1. The top diagnoses that did require rheumatology follow-up were joint pain, rheumatoid arthritis (RA), and +ANA, whereas those that did not require an in-person follow-up were joint pain, +ANA, and fibromyalgia. The current median wait for a new in-person rheumatology appointment in our division is 80 days compared to a 30 day wait time for a new patient video triage appointment.
Conclusion: Through a new patient video triage program for rheumatology patients, we have shown that only 25% of the video patients needed a subsequent in-person rheumatology follow up. The referral sources and most common reason for visit were similar between the 2 groups. Of note, the average wait time for a video triage appointment is less than half of an in-person new patient appointment. Given these findings, we plan to continue this successful new patient video program to help facilitate more timely initial rheumatology evaluation and facilitate more appropriate in-person rheumatology visits.
To cite this abstract in AMA style:
Sharma D, Dore A, Rossi C, Heintzinger J. Successful Implementation of a New Patient Video Triage Program [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/successful-implementation-of-a-new-patient-video-triage-program/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/successful-implementation-of-a-new-patient-video-triage-program/