Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
Ethnic disparities in outcomes of
RA patients have been attributed to delayed presentation to specialty care and
access to DMARDs, greater disease burden, and less years of education. Recent
literature supports a role for socioeconomic status (SES) as a determinant of
RA disease status, including clinical disease activity measures, mortality, seropositivity,
and treatment delays. The purpose of this analysis was to delineate the
association of SES versus race/ethnicity with RA autoantibody status in a
diverse cohort of RA patients.
Methods:
Ethnic Minority RA Consortium
(EMRAC) participants with recorded anti-CCP positive markers at time of
enrollment visit were abstracted for analysis; demographics (age, gender, race,
years of education), clinical features (tobacco use, erosions, disease duration),
and clinical outcomes (RAPID3) were also abstracted. An estimate of SES
was derived from the median housing income of the city of each enrollment site.
Median incomes less than two-fold the 2014 poverty line ($47,700) defined lower
SES status. Logistic regression was used to model risk factors and their
association with positive anti-CCP.
Results:
346 EMRAC participants with
self-reported race/ethnicity were abstracted for analysis; 284 (82%) were
female. The average values for the following parameters were: age 56.1
(±15.6) years, disease duration 9.4 (±10.1) years, and education 13.8 (±3.7)
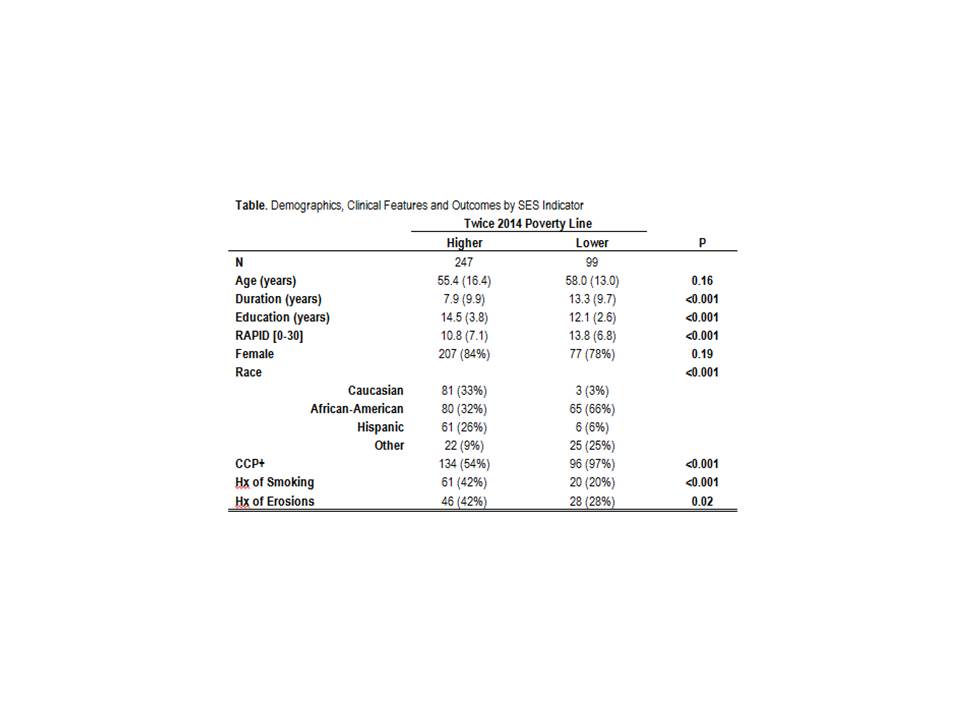
years. Ninety-nine (28.6%) of EMRAC participants were enrolled at sites
servicing lower than the twice poverty line. With this SES indicator,
significant differences in participants’ disease duration, education years,
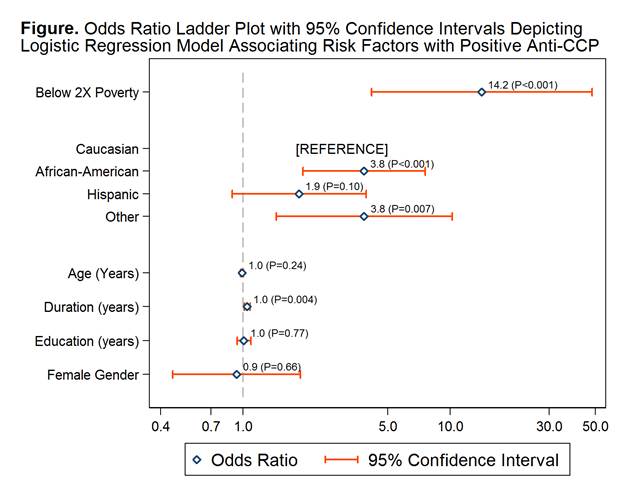
clinical features, and outcomes were observed (Table). In logistic
regression modelling, being below the twice poverty line was significantly
associated with the presence of anti-CCP [13-fold increase; odds ratio=14.2] (Figure).
Both African-American and other race participants also had increased odds of
the presence of anti-CCP compared to Caucasian subjects, but less than that for
low SES. Tobacco use and erosions could not be modeled due to missing
clinical data. However, in a full model with both smoking and erosion
indicators, lower SES remained the strongest risk factor associated with
positive anti-CCP.
Conclusion:
In a diverse ethnic cohort,
disparity in income as an estimate of SES was a stronger risk factor of RA
autoantibody status than race/ethnicity. As autoantibody status is a poor
prognosticator, policies that improve access to specialty care and RA
medications must be paralleled by improvements in overall SES of individuals in
order to minimize the impact of disease.
To cite this abstract in AMA style:
Quinones M, Dowell S, Kerr GS, Swearingen C, Yazici Y, Espinoza L, Garcia-Valladares I, Treadwell EL, Lawrence Ford T, Scherrer Y, Mosley-WIlliams A, Perez Alamino R, Ince A, Amatruda J, Flautero Arcos J. Socioeconomic Status, Ethnicity/Race, and Autoantibody Status in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/socioeconomic-status-ethnicityrace-and-autoantibody-status-in-rheumatoid-arthritis/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/socioeconomic-status-ethnicityrace-and-autoantibody-status-in-rheumatoid-arthritis/