Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic sclerosis (SSc) is a multisystem autoimmune disease with heterogeneous manifestations and significant impairment in health-related quality of life (HRQoL). SSc outcomes are shaped by biological, clinical, sociodemographic, and psychosocial factors, with well-documented disparities by race, sex, and socioeconomic status. While clinical contributors to HRQoL are established, the role of community-level deprivation remains understudied in SSc.
Methods: We analyzed data from 314 adult patients with SSc who met 2013 ACR/EULAR classification criteria and were enrolled in a longitudinal observational cohort at the Medical University of South Carolina. HRQoL was measured using the SF-36 Physical (PCS) and Mental (MCS) Component Summary scores. We examined associations between HRQoL scores and sociodemographic factors, clinical characteristics, and community deprivation indices – Area Deprivation Index (ADI) and Environmental Justice Index Social-Environmental Rank (EJI-SER). ADI, evaluated at the census block level, was assessed using national percentiles and state deciles to reflect neighborhood-level disadvantage. EJI-SER, evaluated at the census tract level, captured cumulative environmental and social vulnerability. Bivariate comparisons and multivariable linear regression were used to estimate associations with PCS and MCS scores.
Results: Among 314 SSc patients (44.6% limited cutaneous, 48.1% diffuse cutaneous, 7.3% sine), significant differences by SSc subtype were observed for race, gender, modified Rodnan skin score (mRSS), forced vital capacity (FVC), esophageal stricture, and history of renal crisis (Table 1). Average PCS and MCS scores varied significantly across demographic, clinical, and socioeconomic factors (Figure 1). In multivariable linear regression analysis (Figure 2), lower PCS was associated with Black race (β=–4.08, p=0.002), public insurance (β=–5.65, p< 0.001), disability (β=–5.69, p=0.01), and depression (β=–5.17, p=0.001), while higher education was protective (β=8.40, p=0.02). Higher (worse) deprivation scores for ADI (state β=–1.09, p< 0.0001; and national rank β=–0.10, p=0.0002), and EJI-SER (β=–0.73, p=0.005) were associated with worse PCS. For MCS, depression (β=–0.83, p< 0.0001), current smoking (β=–6.32, p=0.01), and ADI national rank (β=–0.06, p=0.03) were significantly associated. A range of additional clinical variables, including measures of pulmonary, gastrointestinal, and renal involvement, also demonstrated associations with HRQoL scores (Figure 2).
Conclusion: Both individual- and community-level social determinants contribute meaningfully to disparities in HRQoL among patients with SSc. Consistent with prior literature, factors associated with more severe disease—such as organ involvement, Black race, lower educational attainment, public insurance, smoking, and depression—were linked to lower HRQoL. Notably, this is the first study to demonstrate that higher ADI and EJI-SER scores, reflecting neighborhood-level deprivation, are associated with worse HRQoL in SSc. These indices may offer novel tools for identifying at-risk populations and guiding equity-focused care strategies.
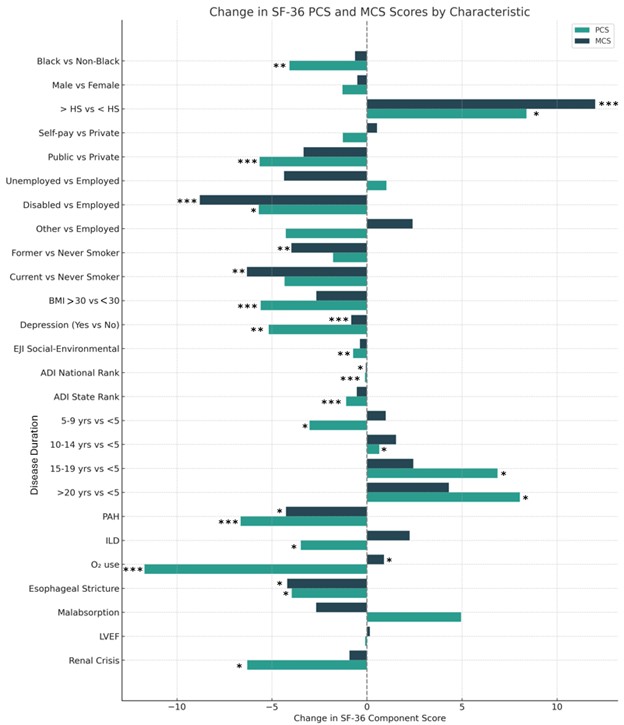 Table 1. Patient Characteristics by Systemic Sclerosis Subtype.
Table 1. Patient Characteristics by Systemic Sclerosis Subtype.
Values are presented as number (percentage) for categorical variables and mean ± standard deviation (SD) for continuous variables. Comparisons are shown across limited cutaneous (lcSSc), diffuse cutaneous (dcSSc), and sine scleroderma subtypes. Abbreviations: ADI = Area Deprivation Index; EJI-SER = Environmental Justice Index Social-Environmental Rank; FVC = forced vital capacity; Hx = history.
.jpg) Figure 1. Heatmap of Average PCS and MCS Scores by Patient Characteristics and Social Factors.
Figure 1. Heatmap of Average PCS and MCS Scores by Patient Characteristics and Social Factors.
This heatmap displays mean Physical Component Summary (PCS) and Mental Component Summary (MCS) scores across demographic and socioeconomic subgroups among patients with systemic sclerosis. Darker shading indicates higher (better) average quality of life scores. An asterisk (*) indicates that the subgroup belongs to a characteristic category with a statistically significant association (p < 0.05) with PCS or MCS. Abbreviations: PCS = Physical Component Summary; MCS = Mental Component Summary; SSc = Systemic sclerosis; HS = High School; Ins = Insurance; BMI = Body Mass Index.
.jpg) Figure 2. Estimated Changes in SF-36 Physical and Mental Component Scores by Characteristic.
Figure 2. Estimated Changes in SF-36 Physical and Mental Component Scores by Characteristic.
This figure illustrates the estimated differences in Physical Component Summary (PCS) and Mental Component Summary (MCS) scores associated with clinical, demographic, and social factors among patients with systemic sclerosis. Bars represent beta coefficients for predicted change in PCS and MCS scores from multivariable linear regression analysis. Asterisks indicate statistical significance (*p < 0.05, **p < 0.01, ***p < 0.001). Abbreviations: PCS = Physical Component Summary; MCS = Mental Component Summary; SSc = Systemic sclerosis; EJI = Environmental Justice Index; ADI = Area Deprivation Index; LVEF = Left ventricular ejection fraction; PAH = Pulmonary arterial hypertension; ILD = Interstitial lung disease.
To cite this abstract in AMA style:
Smith S, Ramos P, Wilson D, Kamen D, Silver R. Sociodemographic, Clinical, and Community-Level Deprivation Factors are Associated with Health-Related Quality of Life in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/sociodemographic-clinical-and-community-level-deprivation-factors-are-associated-with-health-related-quality-of-life-in-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sociodemographic-clinical-and-community-level-deprivation-factors-are-associated-with-health-related-quality-of-life-in-systemic-sclerosis/