Session Information
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: High placebo response rates have challenged interpretation of clinical trial results in SLE and may have contributed to failure of some effective treatments. One hypothesis to explain inflated placebo responses is that patients may not have sufficient disease activity at baseline. Most SLE study designs require a score of ≥6 on the SLE Responder Index (SLEDAI) at entry. Some have attempted to enrich for more active disease by adding an additional inclusion criterion for score A (severe) in ≥1 organ system and/or B (moderate) in ≥2 organ systems on the British Isles Lupus Assessment Group (BILAG) index (at least 1 BILAG A or 2 B). However, the impact of this requirement on enrollment and study outcomes, including placebo response has not been previously examined.
Methods: Data from completed Phase II and III SLE trials that enrolled ≥100 subjects and reported endpoints using SLEDAI and/or BILAG (SRI-4 and/or BICLA responses) were included in the analysis. In trials that did not require minimal BILAG scores, the proportions of patients who had at least 1 BILAG A or 2 B scores at baseline were examined. Trials that included the BILAG requirement were compared to those that did not for recruitment rates, meeting primary endpoint, and placebo SRI-4 and BICLA response rates.
Results: Thirty (16 Phase II and 14 Phase III) trials met the initial search criteria; one was excluded from the analysis because patients with BILAG A at screening were not allowed. Most of the studies (70%) required SLEDAI score ≥6 at entry; 15 (51.7%) trials required at least 1 BILAG A or 2 B scores and 14 (48.9%) did not. In studies with no BILAG requirement, the mean percent of patients with at least 1 BILAG A or 2 B scores was 61.1%.
Mean/median recruitment rates for all 29 studies combined were 0.25/0.21 patients/site/month (p/s/m). Trials with no BILAG requirement enrolled twice as fast as the ones that required at least 1 BILAG A or 2 B scores: mean/median recruitment rates 0.34/0.26 p/s/m versus 0.17/0.14 p/s/m (p< 0.05, Figure 1).
Eleven out of the 29 (39.7%) trials met the primary endpoint; average SRI-4 and BICLA placebo response rates were 44.4% and 34.8% respectively. More studies with no BILAG requirement met their primary endpoint and had lower means of placebo response for both SRI-4 and BICLA than the trials with at least 1 BILAG A or 2 B scores required (Figure 2).
Conclusion: It has been hypothesized that adding minimal BILAG requirement to the traditional SLEDAI criterion at entry will increase the probability of positive outcomes and decrease the inflated placebo response seen in trials of SLE. However, results from the completed studies suggest the opposite: at least 1 BILAG A or 2 B scores requirement at entry was associated with higher placebo response rates and lower likelihood of meeting the primary endpoint, and at the same time, significantly lower enrollment rates. This unexpected finding merits further investigation.
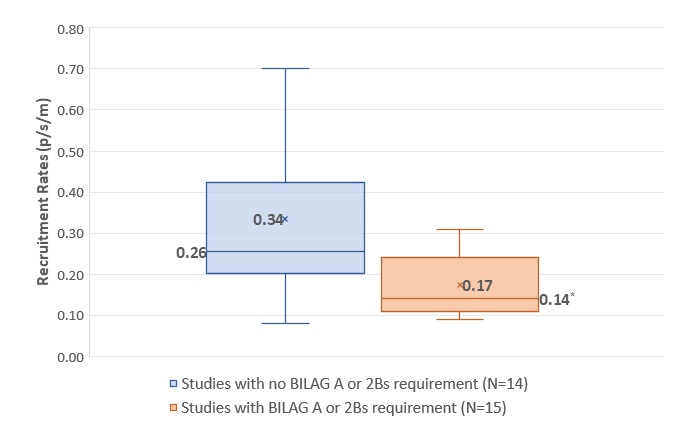 Figure 1: Impact of at least 1 BILAG A or 2 B scores requirement on recruitment rates: comparison of recruitment rates (patients/site/month) of trials that had this requirement with the ones that di not (*p < 0.05, Mann-Whitney Rank Sum)
Figure 1: Impact of at least 1 BILAG A or 2 B scores requirement on recruitment rates: comparison of recruitment rates (patients/site/month) of trials that had this requirement with the ones that di not (*p < 0.05, Mann-Whitney Rank Sum)
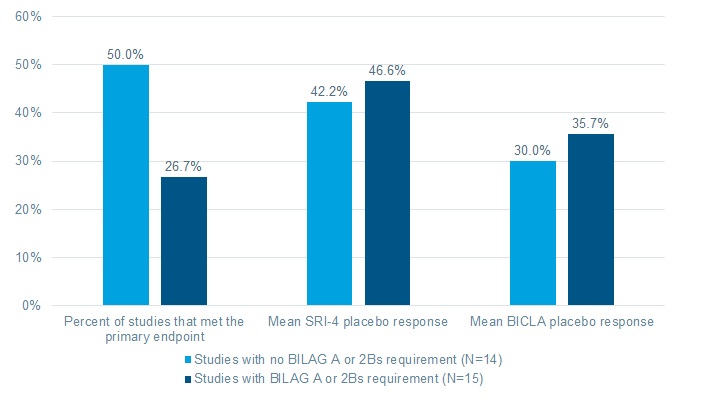 Figure 2: Impact of adding 1 BILAG A or 2 B scores requirement as inclusion on study outcomes: Percent of studies that met their primary endpoint and mean proportions of placebo patients achieving SRI_4 and BICLA responses.
Figure 2: Impact of adding 1 BILAG A or 2 B scores requirement as inclusion on study outcomes: Percent of studies that met their primary endpoint and mean proportions of placebo patients achieving SRI_4 and BICLA responses.
To cite this abstract in AMA style:
Olech E, Hussain F, Merrill J. Should SLE Patients Entering Clinical Trials Be Required to Have at Least One BILAG A and/or Two BILAG B Domain Scores? [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/should-sle-patients-entering-clinical-trials-be-required-to-have-at-least-one-bilag-a-and-or-two-bilag-b-domain-scores/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/should-sle-patients-entering-clinical-trials-be-required-to-have-at-least-one-bilag-a-and-or-two-bilag-b-domain-scores/