Session Information
Date: Monday, November 11, 2019
Title: 4M118: Reproductive Issues in Rheumatic Disorders (1896–1901)
Session Type: ACR Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Pregnancy in patients with SLE is associated with significant morbidity and mortality. SLE activity during pregnancy, specifically nephritis, makes the differential diagnosis with preeclampsia (PE) troublesome in clinical practice. The use of angiogenic factors, like vascular endothelial growth factor (VEGF) and placental growth factor (PlGF), and antiangiogenic factors, such as soluble Fms-like tyrosine kinase-1 (sFlt-1), has been proposed to help differentiate these two conditions, but there is no available data about these cytokines in this scenario. The objective of this study was to evaluate circulating levels of VEGF, PlGF and sFlt-1 in SLE pregnant women with inactive disease, active lupus nephritis and PE.
Methods: Patients with SLE (ACR criteria) with singleton pregnancies followed at a high risk prenatal care, without any other autoimmune disease, were included. They were divided according to disease activity using SLEPDAI (SLE Pregnancy Disease Activity Index), clinical and laboratory evaluation by a rheumatologist experienced in evaluating pregnant SLE patients and the occurrence of PE. Blood samples were collected at the third trimester of pregnancy, within 3 weeks of delivery, and frozen for subsequent blinded analysis by ELISA kits (PlGF – DRG Instruments, Marbug, Germany; sFlt-1 and VEGF – R&D systems, Minneapolis, United States).
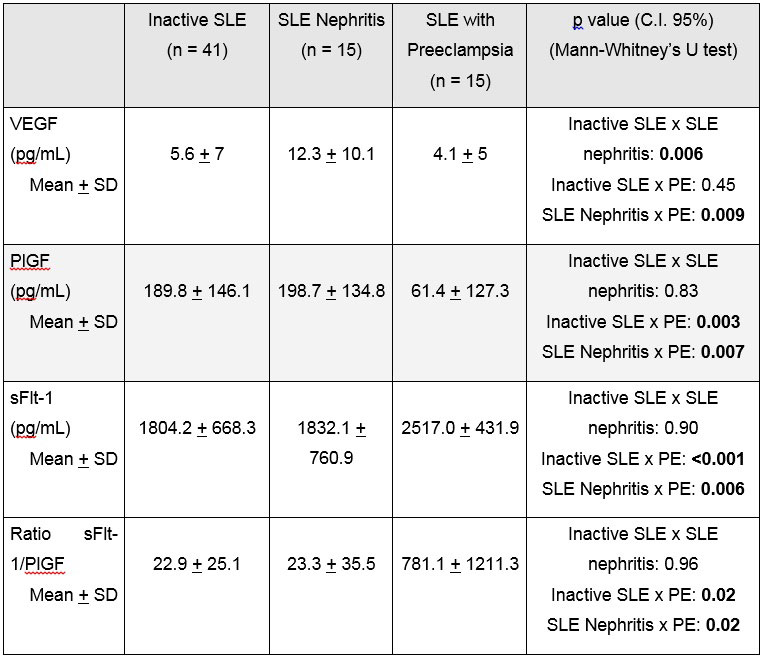
Results: Seventy one women were included. Forty one patients had inactive SLE (Group 1, SLEPDAI < 4), 15 had active lupus nephritis (Group 2, SLEPDAI >4, including renal criteria) and 15 had PE (Group 3). Mean gestational age at blood collection was of 36.8, 33.7 and 34.5 weeks, respectively and delivery at 38.7, 35.7 and 35.8 weeks, respectively; statistically significantly higher in patients with inactive SLE (Table 1). Mean levels of VEGF, PlGF and sFlt-1 of each group are reported on Table 2. Patients with SLE and PE had statistically significantly lower mean serum levels of PlGF than SLE patients without PE, while sFlt-1 was significantly higher in patients with PE compared to pregnant patients with inactive SLE or lupus nephritis. The sFlt-1/PlGF ratio was also significantly higher in patients of Group 3 (PE) compared to other patients with SLE (Groups 1 and 2). VEGF was higher in patients with SLE nephritis compared to inactive SLE and SLE with PE, while PlGF and sFlt-1 were similar when both groups without PE were compared.
Conclusion: In this study, pregnant SLE patients with PE had similar angiogenic and antiangiogenic profile of patients with PE without SLE – low PlGF and high sFlt-1, with high sFlt-1/PlGF ratio. This pattern differs from patients with inactive SLE or active lupus nephritis, the main differential diagnosis during gestation. Evaluation of angiogenic and antiangiogenic factors, specially PlGF and sFlt-1, can be a new tool to differentiate PE from lupus nephritis during pregnancy in clinical practice.

To cite this abstract in AMA style:
De Jesus G, Lacerda M, Rodrigues B, dos Santos F, Nascimento A, Porto L, Ramires de Jesús N, Levy R, Klumb E. sFlt-1, PlGF and VEGF in the Differential Diagnosis Between Active SLE Nephritis During Pregnancy and Preeclampsia [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/sflt-1-plgf-and-vegf-in-the-differential-diagnosis-between-active-sle-nephritis-during-pregnancy-and-preeclampsia/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sflt-1-plgf-and-vegf-in-the-differential-diagnosis-between-active-sle-nephritis-during-pregnancy-and-preeclampsia/