Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: It is established that autoimmune diseases are more common in females than males. Large scale idiopathic inflammatory myopathy (IIM) registries have shown a similar pattern of female predominance. However, inflammatory myopathies have a wide variability of clinical manifestations and it remains unclear if differences in prevalence leads to different phenotypes and thus, a different medication response, between males and females. We aim to compare differences in antibody profile, organ involvement, frequency of comorbidities, and treatment response between male and female patients with IIM.
Methods: A registry was created of Montefiore Medical Center patients that met 2017 EULAR/ACR classification criteria for IIM. Demographics, IIM subtype, clinical manifestations, comorbidities, and treatment history were documented. Interstitial lung disease (ILD) presence, progression, and severity were determined by CT and pulmonary function tests. Medication failure was defined by rheumatologist, discontinuation due to adverse effects, or medication change within 3 months. Medication control was defined by documented clinical improvement. Statistical analyses included Chi-square and Fisher’s Exact test.
Results:
The cohort consisted of 152 patients, of which 114 (75%) were women and 38 (25%) were men. 25% of cohort was of Latin ethnicity and races represented included African American (53%), Caucasian (34%), Asian (4%), and American Indian (2%).
The distribution of myositis exhibited was predominantly female, as expected, except IBM was more prevalent in males (27% vs 7%, p=0.008). Antibody profiles revealed men had increased frequency of NXP2 (21% vs 2%, p= 0.0443) while the rest of antibodies were similarly distributed between the sexes.
There were no significant sex differences in frequencies of DM skin manifestations, except the holster sign was not documented in men. Prevalence, severity, and progression of ILD were similar (Table 1). The frequency of neoplasms, HTN, HLD, and GERD were evenly distributed. However, 17 (19%) females patients had osteoporosis while only 1 (3%) male patient was had osteoporosis (p= 0.039). 29% of women had a single secondary autoimmune condition in comparison to 10% of men (p value = 0.0279).
Comparison of treatments revealed patients, regardless of sex, had less disease control with AZA and MTX, yet MMF and Rituximab had increase rates of control (Table 2). Men achieved less disease control with HCQ in comparison to women (p value =0.034). 35 (31%) of women had limited, low dose exposure to steroids while 0 (0%) of men were exposed to similar length and dosing of steroids (p value =0.0006). Yet, 18% of men had increased exposure to chronic, high dose steroids in comparison to 3% of women (p value= 0.003).
Conclusion: Although antibody profiles and clinical presentations between the sexes were similar, men had less disease control with MTX and were exposed to increased dose and length of steroid treatment. Women had shorter time and smaller dose exposure to steroids, yet steroid damage was still evident. This retrospective chart review was limited by small sample sizes but differing medication responses and prescriber patterns between sexes in IIM warrants further investigation.
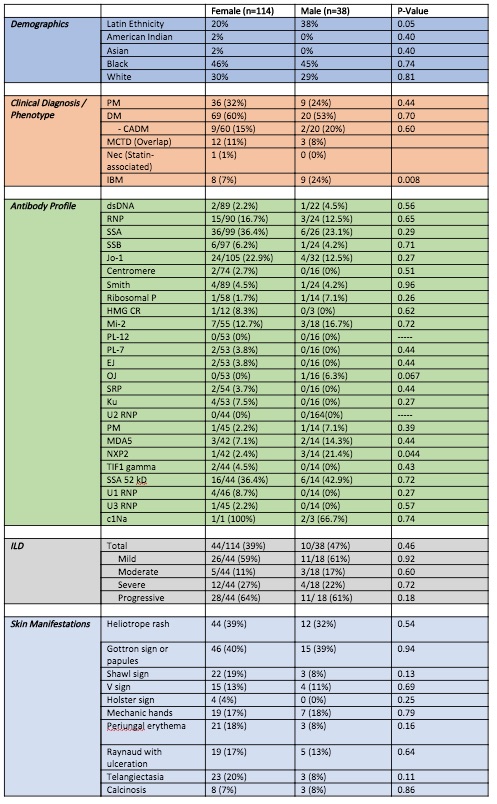 Table 1. Similarities in demographics, antibody profile, and clinical manifestations among men and women with IIM.
Table 1. Similarities in demographics, antibody profile, and clinical manifestations among men and women with IIM.
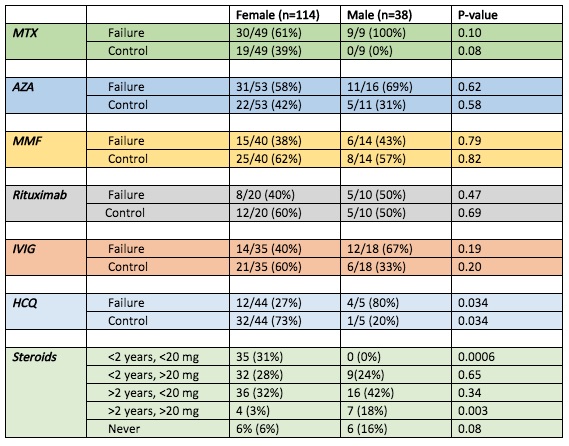 Table 2. Differences in medication response and steroid exposure between males and females with IIM.
Table 2. Differences in medication response and steroid exposure between males and females with IIM.
To cite this abstract in AMA style:
Valle A, Law J, Mullins K, Mahmood S. Sex Differences in Antibody Profile, Phenotype, and Treatment Response in a Racially Diverse Population with Idiopathic Inflammatory Myopathies [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/sex-differences-in-antibody-profile-phenotype-and-treatment-response-in-a-racially-diverse-population-with-idiopathic-inflammatory-myopathies/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sex-differences-in-antibody-profile-phenotype-and-treatment-response-in-a-racially-diverse-population-with-idiopathic-inflammatory-myopathies/