Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: GCA and PMR are closely related inflammatory diseases. The diagnostic criteria of both disorders depend on a combination of clinical features and elevated ESR or CRP levels. ESR and CRP are also used to monitor disease activity. These biomarkers, however, are not disease specific and not consistently elevated in all GCA and PMR patients. Previously, serum levels of IL-6, SAA and calprotectin were found to be increased in small scale cross-sectional GCA and PMR studies. Calprotectin expression was also found in neutrophils and macrophages in temporal artery biopsies (TABs) of GCA patients. The aim of this study was to identify and compare the values of IL-6, SAA and calprotectin as biomarkers for diagnosing GCA and PMR, monitoring disease activity and predicting disease course.
Methods: Serum concentrations of IL-6, SAA and calprotectin were determined by ELISA in 36 newly diagnosed GCA patients (C-GCA (TAB+) or LV-GCA (PET/CT+)) and 27 newly diagnosed PMR patients (fulfilling the Chuang-Hunder criteria), before start of glucocorticoid treatment. Thirty age- and sex matched healthy controls were included as well. Follow-up sera from patients were tested again 3 months (n= 21 for GCA and n= 21 for PMR) and 1 year (n= 23 for GCA and n= 16 for PMR) after the start of treatment. TABs (n=17) from GCA patients were stained with anti-calprotectin and anti-CD15 by immunohistochemistry.
Results: Baseline levels of IL-6, SAA and calprotectin in GCA and PMR patients were higher compared to healthy controls. Treatment decreased the levels of IL-6 and SAA in both GCA patients and PMR patients, but serum levels of calprotectin decreased in PMR patients only. Relapse free survival between the groups with relatively low and high levels of the serum markers did not differ. IL-6 correlated with CRP, and SAA correlated with both CRP and ESR. Calprotectin did not correlate with IL-6, SAA, CRP or ESR, suggesting an IL-6 independent pathway. Interestingly, calprotectin levels were also elevated in GCA and PMR patients with normal ESR or CRP levels. Immunohistochemical staining of TABs showed calprotectin expression in all TABs (Fig. 1). Only a minority of calprotectin positive cells were CD15+ neutrophils.
Conclusion: Serum levels of IL-6, SAA and calprotectin discriminate GCA and PMR patients from healthy controls at the group level. In addition, serum levels of IL-6 and SAA decrease with treatment induced remission in GCA and PMR patients. None of the biomarkers tested at baseline predicted future relapse. Serum calprotectin could be a potential marker for silent ongoing vascular inflammation in GCA patients. The diagnostic value of serum IL-6, SAA and especially calprotectin as biomarkers should be further examined and validated.
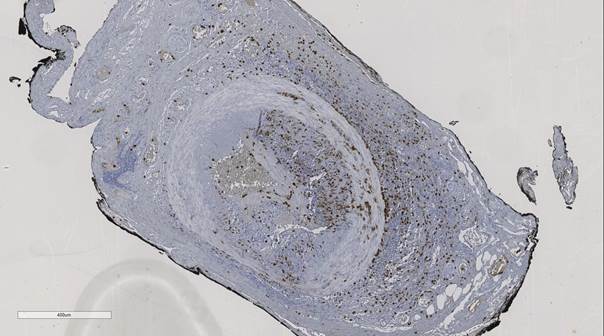
Fig. 1: Calprotectin expression in the TAB of a GCA patient (DAB/brown).
To cite this abstract in AMA style:
van Sleen Y, Hoekstra M, Bijzet J, Abdulahad WH, Boots AMH, Brouwer E. Serum IL-6, SAA and Calprotectin As Biomarkers in Giant Cell Arteritis and Polymyalgia Rheumatica [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/serum-il-6-saa-and-calprotectin-as-biomarkers-in-giant-cell-arteritis-and-polymyalgia-rheumatica/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/serum-il-6-saa-and-calprotectin-as-biomarkers-in-giant-cell-arteritis-and-polymyalgia-rheumatica/