Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Women with Systemic lupus erythematosus (SLE) have more difficulty in achieving a successful pregnancy than healthy women, because of higher risks for adverse pregnancy outcomes (APOs) especially in preterm birth (1). Many reports revealed that preterm birth is related to uncontrolled high disease activity, including low complements and high titer of anti-double stranded DNA (dsDNA) antibody (2, 3). On the other hand, recently we reported that a relative lower dose of glucocorticoid dose (cut-off dose; 10mg/day) was significantly associated with preterm birth (4). However, it is not clarified whether disease activity parameters or glucocorticoid doses during pregnancy are at greater risk for preterm birth. Therefore, we aimed to identify which disease parameters or glucocorticoid dose may become risk factors for preterm birth.
Methods: We used the data of SLE patients who had been treated at the planning for pregnancy and gave birth from rheumatic disease pregnancy registry in our institution. We collected complement levels (C3, C4, CH50) and the titer of anti-dsDNA antibody at conception as immunological disease activity parameters and glucocorticoid dose during pregnancy. We retrospectively analyzed the association between preterm birth and disease activity parameters or glucocorticoid dose.
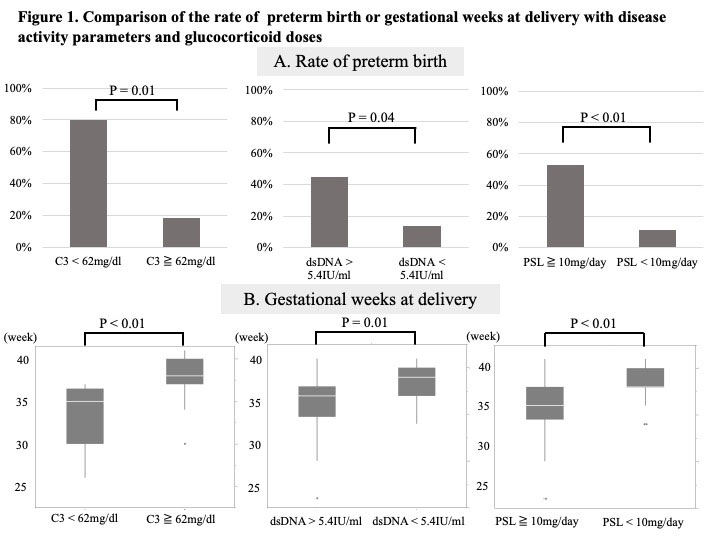
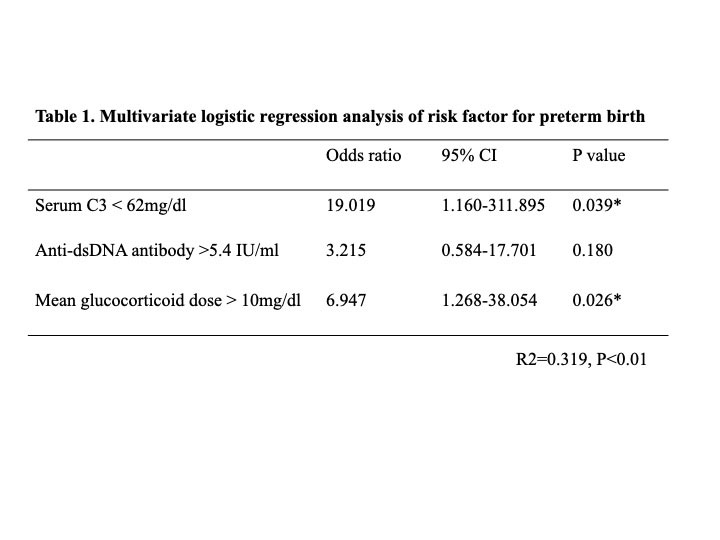
Results: The subjects were 60 pregnancies of 45 patients. Of all cases, preterm birth occurred in 14 cases (23.3%). Preterm birth was associated with C3 levels and the titers of anti-dsDNA antibody (P=0.03 and 0.01). On the other hand, it had no association with C4 and CH50 levels (P = 0.16 and 0.17). We performed logistic regression analysis for preterm birth, which showed that the cut-off of C3 level was 62 mg/dl and that of anti-dsDNA antibody titer was 5.4 IU/ml. We have already showed the cut-off of mean glucocorticoid dose for preterm birth was 10mg/day. Cases with C3 < 62mg/dl or anti-dsDNA antibody > 5.4IU/ml or mean glucocorticoid dose > 10mg/day had an increased risk of preterm birth (P = 0.01, 0.04, < 0.01, respectively, Figure 1). Additionally, gestational weeks at delivery were significantly shorter in these cases (P < 0.01, 0.01, < 0.01, respectively, Figure 1). Multivariate logistic regression analysis of risk factor for preterm birth was performed in Table 1. It showed that C3 < 62mg/dl or mean glucocorticoid dose > 10mg/day was a risk factor for preterm birth (P = 0.039 and 0.026). The combination of C3 < 62mg/dl and mean glucocorticoid dose > 10mg/day had a significantly higher rate of risk for preterm birth (P = 0.01), and significant difference of gestational weeks at delivery (P = 0.02, Figure 2).
Conclusion: In women with SLE, preterm birth is strongly associated with C3 levels and mean glucocorticoid doses. Therefore, it is important to manage both disease activity, especially in C3, and glucocorticoid dose in women who hope to conceive.

To cite this abstract in AMA style:
Shimada H, Wakiya R, nakashima s, Kato M, miyagi t, Ushio Y, Sugihara K, Mino R, mizusaki m, Chujo K, Kameda T, Dobashi H. Serum C3 Level and Glucocorticoid Dose Are Risk Factors for Preterm Birth in Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/serum-c3-level-and-glucocorticoid-dose-are-risk-factors-for-preterm-birth-in-patients-with-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/serum-c3-level-and-glucocorticoid-dose-are-risk-factors-for-preterm-birth-in-patients-with-systemic-lupus-erythematosus/