Session Information
Date: Sunday, October 26, 2025
Title: (0233–0279) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Vogt-Koyanagi-Harada disease (VKH) is a systemic disease that affects the central nervous system, ocular, and integumentary system. It causes bilateral granulomatous uveitis, dysacusia ranging from tinnitus, vertigo to hearing loss, and skin abnormalities such as poliosis, vitiligo, and alopecia. The present criteria only mention tinnitus as an ear finding, despite some studies reporting vestibular and cochlear involvement in individuals with VKH. Also, the diagnostic criteria for VKH do not include hearing loss as an auditory finding
Methods: Our study is one of the unique prospective studies in VKH. We aimed to evaluate the clinical and sub-clinical audio-vestibular (AV) involvement in VKH, and to compare between eye and AV response to treatment. Our patients were recruited and followed for 6 months. All our patients were assessed with emphasis on eye and AV evaluation {using Pure Tone Audiometry (PTA), Transient Evoked Otoacoustic Emission (TEOAE), positioning, spontaneous nystagmus, and caloric tests}. Laboratory investigations included CBC, ALT, AST, Creatinine, ESR, and CRP
Results: 100 patients with VKH were included. 63 cases with Active uveitis: Anterior 23/63 (35.5%), intermediate 10/63 (15.9%), posterior 4/63(6.3%), pan uveitis 35/63 (55.5%). 26 symptomatic patients had symptomatic (clinical) AV involvement either audiological 18/26 (69.2%), vestibular 1/26 (3.8%), or both 7/26 (27%), while 40 asymptomatic patients had subclinical AV involvement: audiological 26/40 (65%), vestibular 2/40 (5%), both 12/40 (30%). The 63 cases with active uveitis, 25/63 (40.3%) had subclinical, and 15/63 (24.2%) had clinical AV involvement. The 37 patients with no uveitis, 14/37 (40.5%) had subclinical and 11/37 (29.7%) had clinical AV involvement. This group with subclinical AV involvement and no eye activity is very important, as without evaluating the AV system, those patients would have been missed without treatment till damage occurs. Patients received treatment according to the activity by different lines of management (Table 1). After 6 months: Follow-up (F/U) for ocular response: Complete response in 33/63 (52.4%), Partial response in 12/63 (19%), No response in 6/63 (9.5%), Worsening in 8/63 (12.7%), Lost F/U in 4/63 (6.3%). Follow up for AV response: subclinical improvement 28/40 (70%), subclinical no improvement 4/40 (10%), subclinical worsening 3/40 (7.5%), lost F/U 5/40 (12.5%), clinical improvement 15/26 (57.7%), clinical no response 6/26 (23.1%), clinical worsening 4/26 (15.4%), lost F/U 1/26 (3.8%). Regarding the group of patients with normal eyes at base line with AV involvement and received treatment: subclinical improvement 10/14 (71.4%), subclinical no improvement 1/14 (7.1%), subclinical worsening 1/14 (7.1%), lost F/U 2/14 (14.3%), clinical improvement 8/11 (72.8%), clinical no response 1/11 (9%), clinical worsening 2/11 (18.2%) (Table 2)
Conclusion: Subclinical AV (40%) involvement is common and more than symptomatic cases and even present in about 40% of cases without uveitis. So, early detection of subclinical AV involvement is important to allow early treatment before damage. We recommend adding AV involvement in the diagnostic criteria of VKH and not only tinnitus
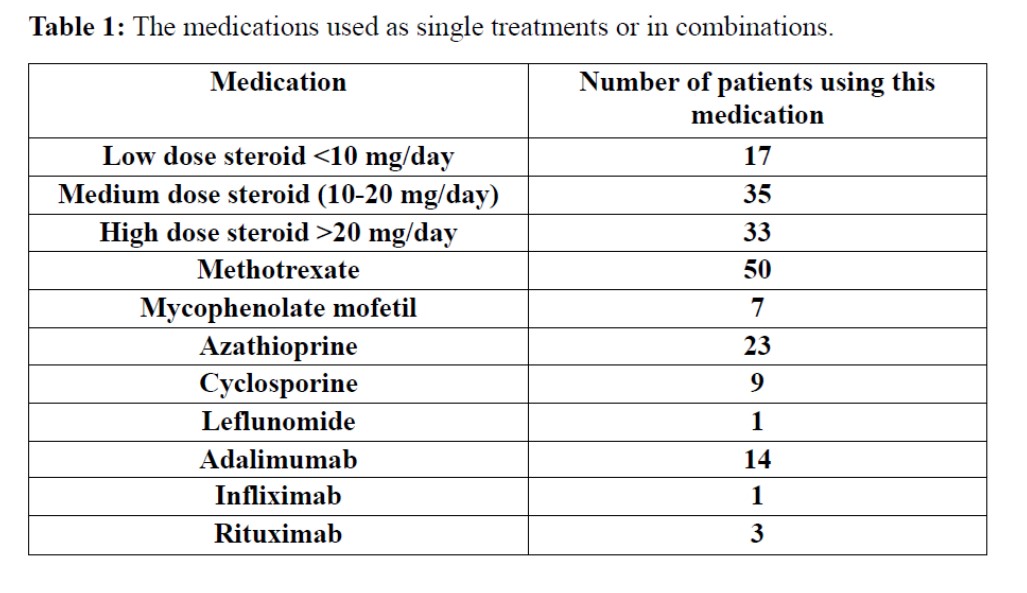 Table 1: The medications used as single treatments or in combinations
Table 1: The medications used as single treatments or in combinations
.jpg) Table 2: Base line characteristics of Uveitis and Audio-vestibular involvement and follow-up
Table 2: Base line characteristics of Uveitis and Audio-vestibular involvement and follow-up
To cite this abstract in AMA style:
Hegazy M, Yacoub R, Sheta S, Amin R, Khalil N. Seeing Beyond the Eye: Subclinical Audio-Vestibular Involvement in Vogt-Koyanagi-Harada Disease [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/seeing-beyond-the-eye-subclinical-audio-vestibular-involvement-in-vogt-koyanagi-harada-disease/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/seeing-beyond-the-eye-subclinical-audio-vestibular-involvement-in-vogt-koyanagi-harada-disease/