Session Information
Session Type: ACR Plenary Session
Session Time: 11:00AM-12:30PM
Background/Purpose: The previously reported prospective, randomizedÐcontrolled MAINRITSAN trial compared rituximab (RTX) to azathioprine (AZA) for maintenance of ANCA-associated vasculitis (AAV) remissions obtained with a combined cyclophosphamide and glucocorticoid (GC) induction regimen. Patients were randomly assigned to receive 500-mg RTX infusions on D1, D15 and 5.5 months later, then every 6 months until 18 months, or AZA for 22 months (initial dose: 2 mg/kg/d). Trial results demonstrated that RTX was superior to AZA at maintaining AAV remission during the planned 28 months of follow-up. We now report the pre-specified long-term outcomes at 60 months of MAINRITSAN trial patients.
Methods: SurvivorsÕ outcomes were ascertained prospectively. Data on survival, relapse, cancers, cardiovascular morbidity and other adverse events were collected from physicians. All patients were analyzed according to randomization group. Quality-adjusted time-without-symptoms-and-toxicity (Q-TWiST) analysis was computed, with the aim of better discerning the therapeutic impact and tradeoffs between treatment toxicity (severe adverse events, SAEs) and disease activity (relapse).
Results: Data from 60 months of follow-up were available for 110 (96%) of the 115 randomized participants. For the RTX- and AZA-treated groups, respectively: 0 and 4 died; 60-month overall survival rates were 100% and 93.0% [95% CI 86.7Ð99.9%] (P=0.045); all-relapseÐfree survival rates were 57.9% [95% CI 46.4Ð72.2%] and 37.2% [95% CI 26.5Ð52.2%] (P=0.012); and major relapse-free survival rates were 71.9% [95% CI 61.2Ð84.6%)] and 49.4% [95% CI 38.0Ð64.3%] (P=0.003). In contrast, no between-group differences were observed for survival without SAEs (P=0.95) and the cumulative GC dose (P=0.11) at 60 months.
For RTX-treated patients, PR3-ANCA positivity or ANCA persistence 12 months after starting maintenance therapy were associated with higher major relapse rates. During the 60-month follow-up, RTX- and AZA-arm patients had similar amounts of time spent with SAEs (P=0.21), whereas the former, compared to the latter, spent 9.7 months less with major relapses (P<0.001) and 12.6 months more without relapse or toxicity (P<0.001). The threshold utility analysis at 60 months showed that the Q-TWiST period was significantly longer for RTX- than AZA-arm patients (55.2 vs. 47.95 months, respectively, P<0.001) (Figure).
Conclusion: This long-term analysis showed that, despite late relapses after the 28-month initial follow-up period, maintenance therapy with RTX remained significantly superior to AZA to maintain remission at 60 months and was associated with better survival. ANCA monitoring seems to be relevant to guide treatment duration. 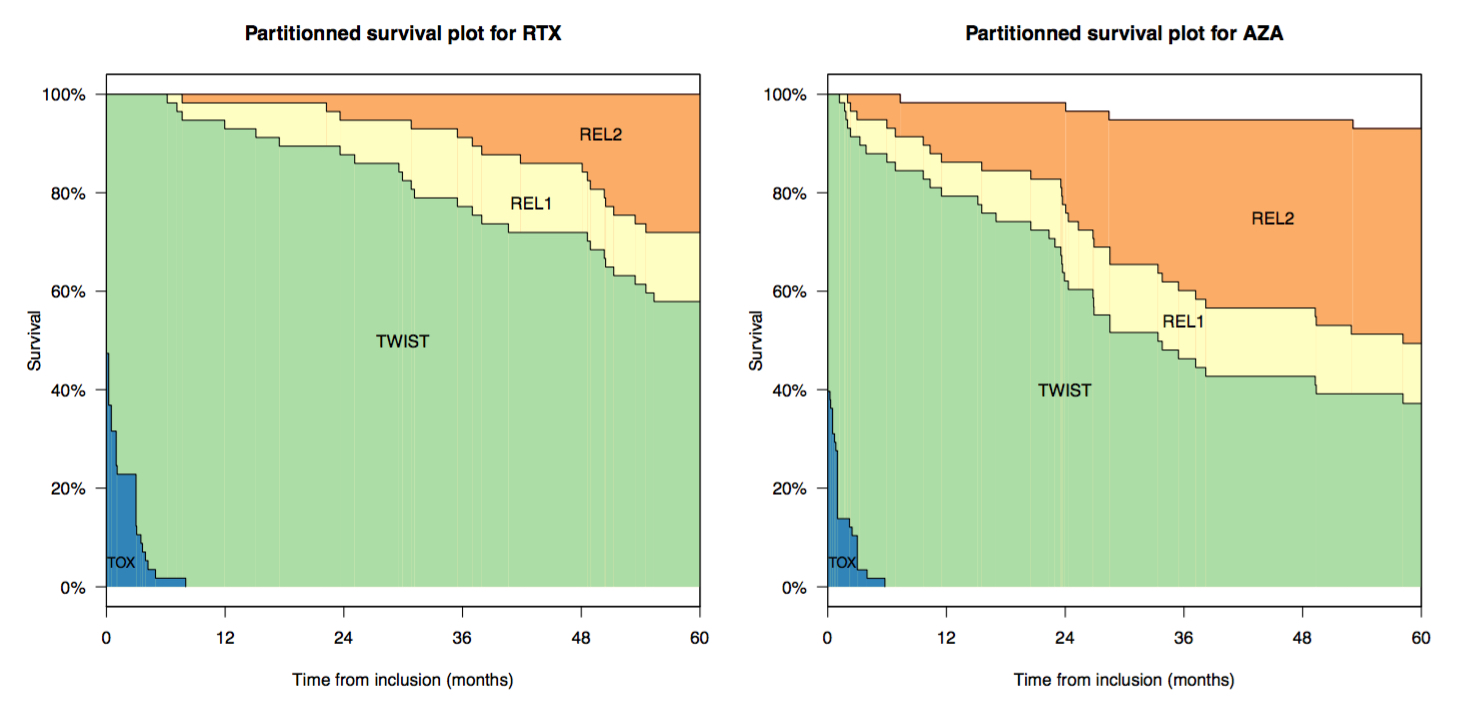
To cite this abstract in AMA style:
Terrier B, Pagnoux C, Perrodeau E, Karras A, Khouatra C, Aumaître O, Cohen P, Maurier F, Decaux O, Desmurs-Clavel H, Gobert P, Quémeneur T, Blanchard-Delaunay C, Godmer P, Puéchal X, Mouthon L, Ravaud P, Guillevin L. Rituximab Versus Azathioprine to Maintain Remission of ANCA-Associated Vasculitides (MAINRITSAN): Follow-up at 60 Months [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/rituximab-versus-azathioprine-to-maintain-remission-of-anca-associated-vasculitides-mainritsan-follow-up-at-60-months/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rituximab-versus-azathioprine-to-maintain-remission-of-anca-associated-vasculitides-mainritsan-follow-up-at-60-months/