Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Literature data on the increased risk of severe infection regarding hypogammaglobinemia related to RTX in IMID are controversial and sparse. We proposed to evaluate the risk of severe infections in patients with IMID treated with RTX who presented Ig deficiency (prevalent or acquired).
Methods: We conducted an observational, retrospective single-center study retrieving all patients with at least one infusion of RTX in the department of Rheumatology (CHU Montpellier) between January 1st and December 31st 2017. We included all patients treated for an IMID (rheumatoid arthritis, systemic lupus erythematosus, ANCA-associated vasculitis, primary Sjögren syndrome, inflammatory myopathy, scleroderma, mixt connective diseases, cryoglobulinemia vasculitis and overlap syndrome) with at least one Ig assay performed during follow-up. Patients were followed-up at least12 months after the last infusion of RTX or until the occurrence of a severe infection or death occurring within 12 months after the last infusion of RTX or until the end of the study (May 31st 2020).Ig deficiency was defined as a rate of IgG, and/or IgA and/or IgM lower than the laboratory thresholds. Then, we categorized patients with prevalent Ig deficiency (before the first infusion of RTX), acquired Ig deficiency (normal Ig assays before the first infusion of RTX and with an occurrence of at least one Ig deficiency during follow-up), and patients with normal Ig level from the first infusion to the end of follow-up.
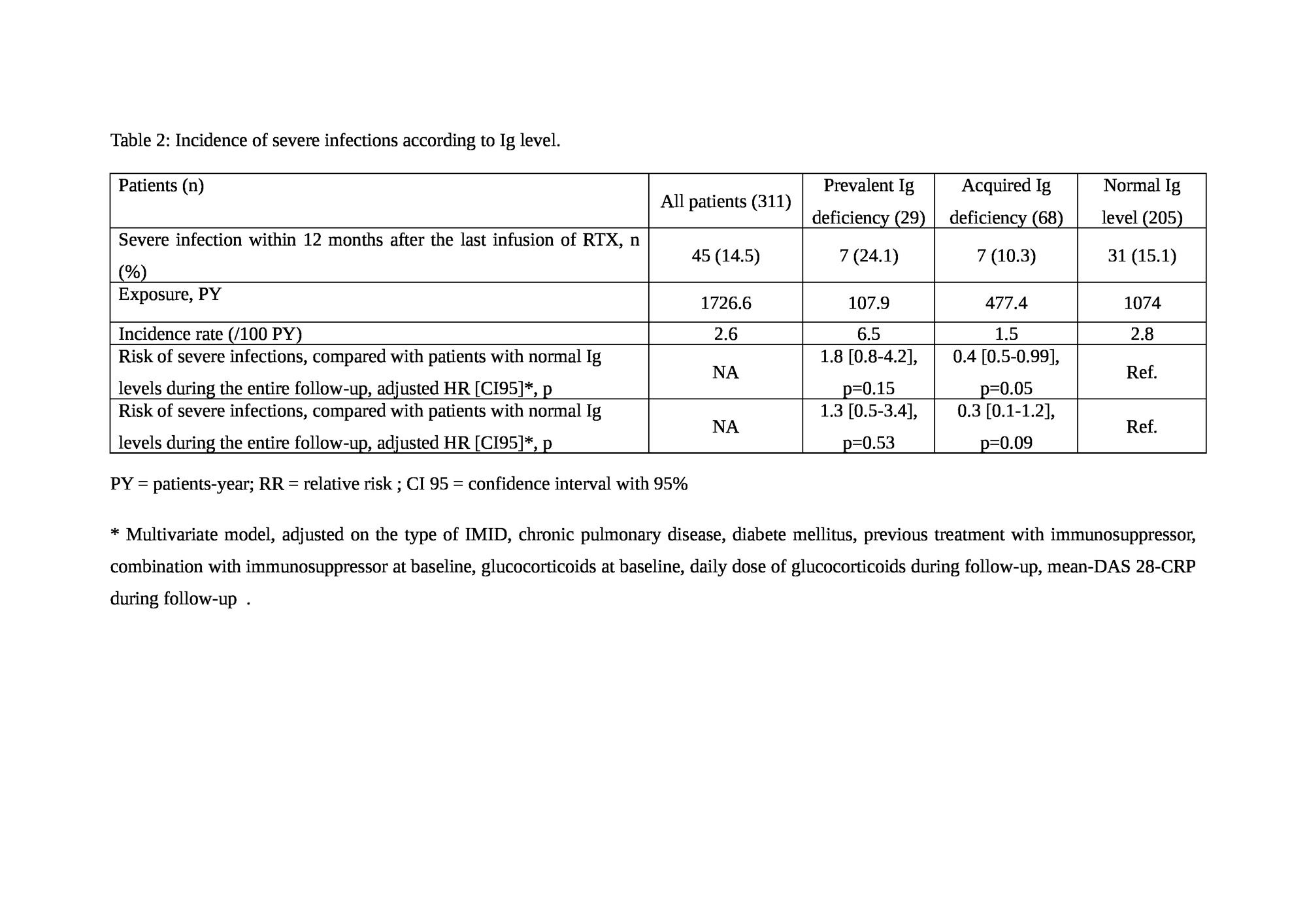
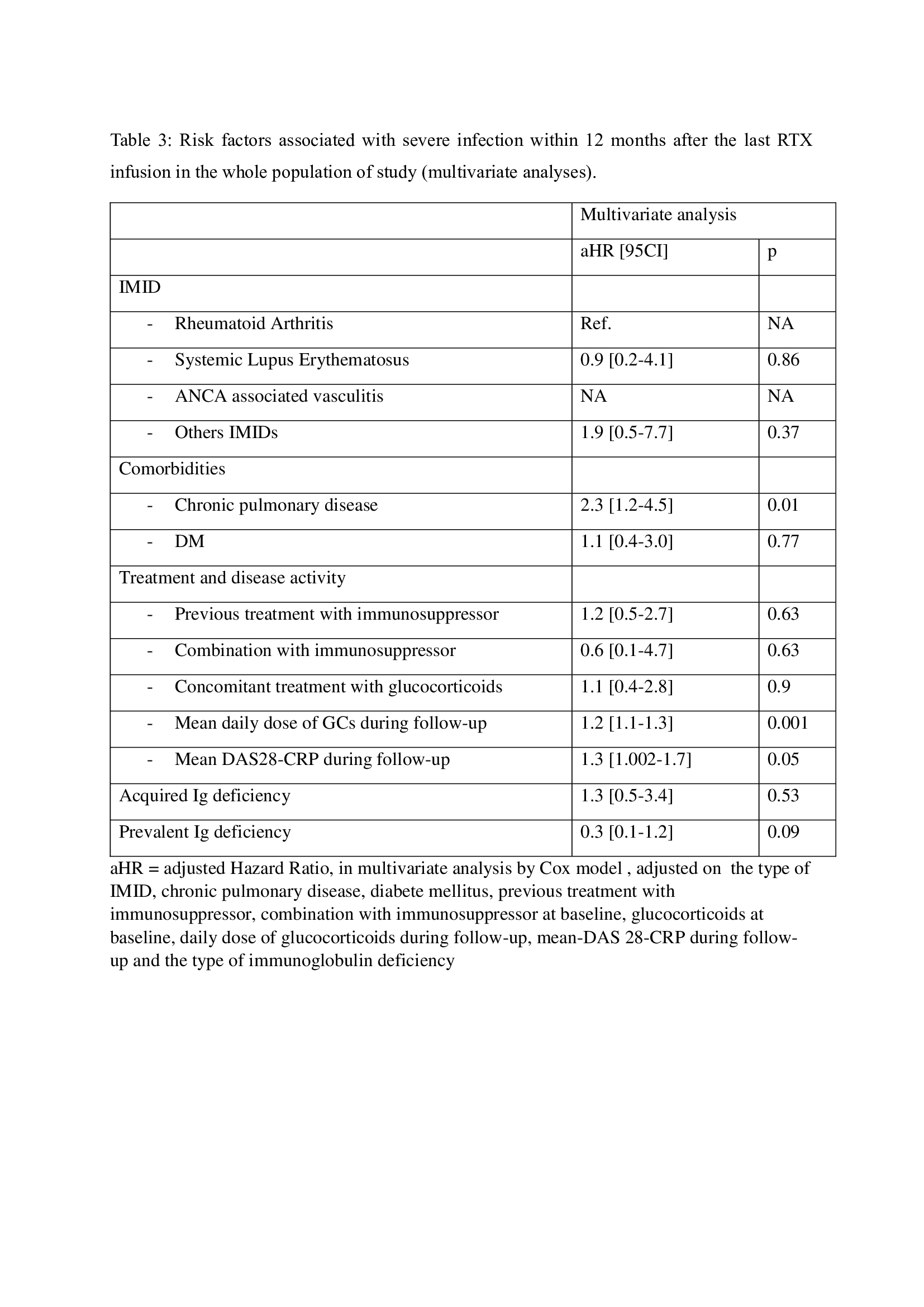
Results: Three hundred and eleven patients were included. Nine patients had undatable Ig deficiency. Twenty-nine patients (9,4%) had prevalent Ig deficiency. As compared with patient with normal Ig level at baseline, concomitant treatment with glucocorticoids (p=0,03) and with a higher daily dose at baseline (p=0,01) were associated with a prevalent Ig deficiency. Sixty-eight patients (22,0%) acquired an Ig deficiency after the first infusion of RTX. A longer time of follow-up and a higher cumulative dose of RTX, the type of IMIDs (SLE and AAV) and concomitant treatment with IS or GCs at baseline, diabetes mellitus and obesity were associated with the occurrence of an Ig deficiency (Table 1). Forty-three patients (14,3%) developed a severe infection within 12 months after the last infusion of RTX. Severe infections occurred more frequently in patients with prevalent Ig deficiency but without any stastistical difference with patient with normal Ig level (Table 2). In multivariate analysis, only chronic pulmonary disease, a higher daily dose of GCs and a higher mean DAS28-CRP during follow-upwere still associated with an increased risk of severe infection (Table 3). In a time-dependant analysis, Ig deficiency in patient treated with RTX, wether acquired or prevalent, was not associated with an increased risk of severe infection (adjusted HR 1.04 [0.5-2.3], p=0.92).
Conclusion: We did not observe an increased risk of severe infection in RTX-induced Ig deficiency. In case of Ig deficiency, RTX management should be discussed on a case-by-case basis, according to an individual assessment of the infectious risk, especially when GCs therapy is used and chronic lung diseases are present.

To cite this abstract in AMA style:
Rempenault C, Lukas C, Tardivon L, Daien C, Combe B, GUILPAIN P, MOREL J. Risk of Severe Infections Associated with Immunoglobulin Deficiency Under Rituximab Therapy in Immune Mediated Inflammatory Diseases [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/risk-of-severe-infections-associated-with-immunoglobulin-deficiency-under-rituximab-therapy-in-immune-mediated-inflammatory-diseases/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-of-severe-infections-associated-with-immunoglobulin-deficiency-under-rituximab-therapy-in-immune-mediated-inflammatory-diseases/