Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Rheumatoid arthritis (RA) therapy is recommended to be intensified according to treat-to-target if DAS28 (disease activity score 28) or CDAI (clinical disease activity index) indicate high/moderate (H/M) activity, although exceptions based on shared decisions are recognized. Comorbid fibromyalgia (FM) and/or depression (DEP) may raise DAS28 and CDAI, independent of inflammation, but often are underrecognized in routine care. A multidimensional health assessment questionnaire (MDHAQ) provides validated feasible screening indices for FM and DEP, FAST4 (fibromyalgia assessment screening tool) (ACR Open Rheum 2019;1:516) and MDS2 (MDHAQ depression screen) (Arth Care & Res 2021;73:120), which agree more than 80% with reference standards, on a single MDHAQ, completed by most patients in 5-10 minutes. We hypothesized that some patients in DAS28-ESR or CDAI H/M vs low/remission (L/R) would have 0 or 1 vs ≥2 swollen joint counts (SJC), but positive vs negative MDHAQ FAST4 and/or MDS2 screens.
Methods: A cross-sectional study at a routine care visit included DAS28 and CDAI. Patients competed an MDHAQ to score patient global assessment, fatigue, 0-3.3 DEP query, self-report 0-54 RADAI painful joint count, 60-symptom checklist (Sx), medical history queries, and FAST4 [positive (+) if 3/4: pain VNS ≥6/10, fatigue VNS ≥6/10, RADAI ≥16/54, and/or Sx ≥16/60] and MDS2 [+ if a 0-3 DEP query is ≥2 or positive DEP on Sx). The numbers of patients in H/M vs L/R DAS28-ESR and CDAI, SJC 0/1 vs ≥2 and FAST4 + vs negative (-) and MDS2+ vs – status were analyzed using chi-square statistics.
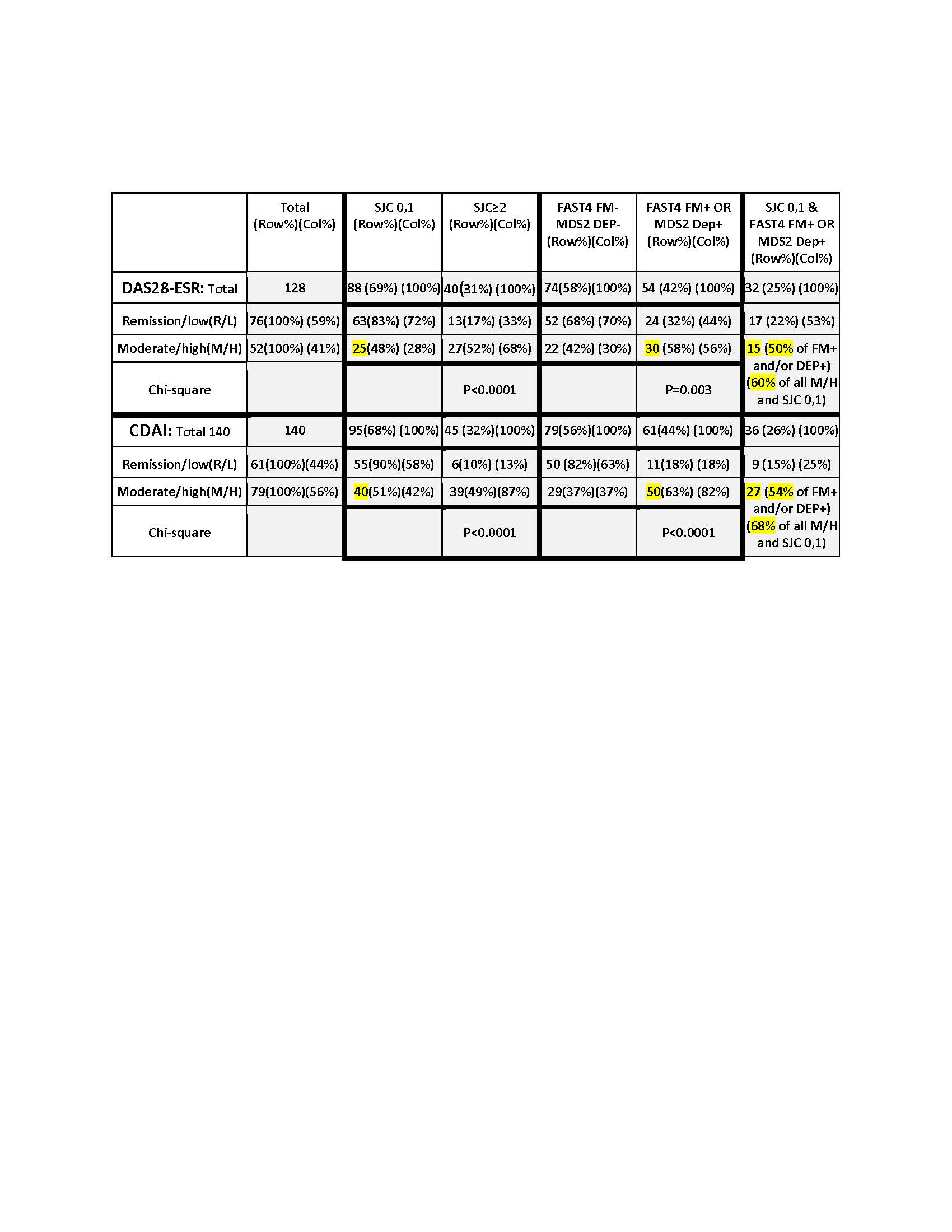
Results: Median age was 61.3 years, median disease duration 10 years, and 75% of patients were female. DAS28-ESR and CDAI M/H vs L/R differed significantly according to SJC, as expected; R/L included 0/1 SJC in 83% of DAS28–ESR and 90% of CDAI (p< 0.001) (Table). However, M/H with 0/1 SJC was seen in 25/52 (48%) by DAS28-ESR and 40/79 (51%) by CDAI. DAS28-ESR and CDAI M/H vs L/R also differed significantly according to FAST4 and MDS2 status, somewhat unexpectedly (Table): 68% of DAS28-ESR L/R were FAST4-,MDS2- while 58% of M/H were FAST4+ &/or MDS2+ (p=0.003); 50/61 (82%) of CDAI L/R were FAST4-,MDS2-, while 50/79 (63%) of M/H patients were FAST4+ &/or MDS2+ (p=< 0.0001) (Table). Patients classified as M/H but with SJC of 0/1 included 15 for DAS28 (50% of 30 M/H and FAST4+ &/or MDS2+, 60% of 25 with M/H and SJC 0/1, and 29% of all 52 M/H patients), and 27 for CDAI (54% of 50 M/H and FAST4+ &/or MDS2+, 68% of 40 with M/H and SJC 0/1, and 34% of all 79 M/H patients) (Table).
Conclusion: Treat-to-target is a useful guideline for most RA patients. However, a sizable majority in H/M DAS28–ESR or CDAI have 0/1 SJC and may not be candidates for therapy escalation. About half of patients with high index scores and 0/1 SJC have comorbid FM or and/or DEP, which can be feasibly screened for with FAST4 and MDS2 indices on a single MDHAQ. Patients with DAS28-ESR or CDAI H/M vs L/R differed significantly in MDHAQ FAST4+ or – and/or MDS2 + or – indices for FM and DEP. Recognition that FM and DEP may elevate RA index scores is analogous to recognition that an elevated ESR may result from a cause other than inflammation. An MDHAQ, completed by most patients in 5-10 minutes, can help rheumatologists interpret RA index scores.
To cite this abstract in AMA style:
Pincus T, Rodwell N, Hunter R. Rheumatoid Arthritis Disease Activity Indices Assess More Than Inflammation: 29%-36% of Patients with Moderate or High DAS28–ESR or CDAI Have 0 or 1 Swollen Joints, but Positive Screens on MDHAQ FAST4 (fibromyalgia Assessment Screening Tool) And/or MDS2 (MDHAQ Depression Screen) Indices [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/rheumatoid-arthritis-disease-activity-indices-assess-more-than-inflammation-29-36-of-patients-with-moderate-or-high-das28-esr-or-cdai-have-0-or-1-swollen-joints-but-positive-screens-on-mdhaq/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatoid-arthritis-disease-activity-indices-assess-more-than-inflammation-29-36-of-patients-with-moderate-or-high-das28-esr-or-cdai-have-0-or-1-swollen-joints-but-positive-screens-on-mdhaq/