Session Information
Date: Monday, November 13, 2023
Title: (1013–1032) Healthcare Disparities in Rheumatology Poster II: Socioeconomic Determinants
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Immune checkpoint inhibitors (ICIs) represent a breakthrough in cancer therapies. However, ICIs may be associated with significant immune-related adverse events (irAEs), including rheumatic irAEs. The frequency, severity, and treatment of rheumatic irAEs are not well characterized among racial and ethnic minorities. Accordingly, we investigated the nature of rheumatic irAEs among patients treated with ICIs and subsequent referrals to rheumatologists at 2 medical centers located in the same geographic region of Los Angeles, both staffed by faculty from the same medical school: Los Angeles General Medical Center (LAG), a safety-net public hospital, and Keck Medical Center (KMC), a private hospital.
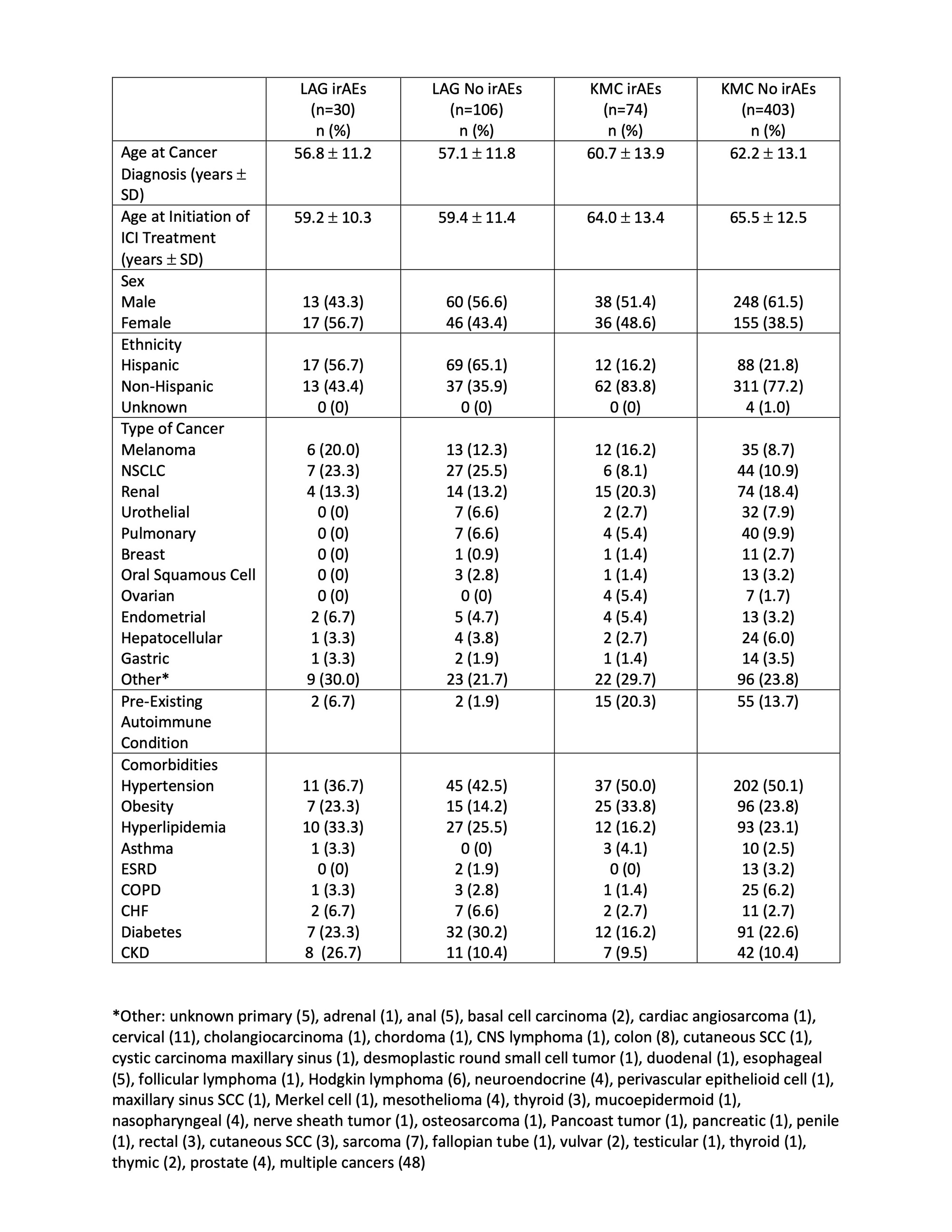
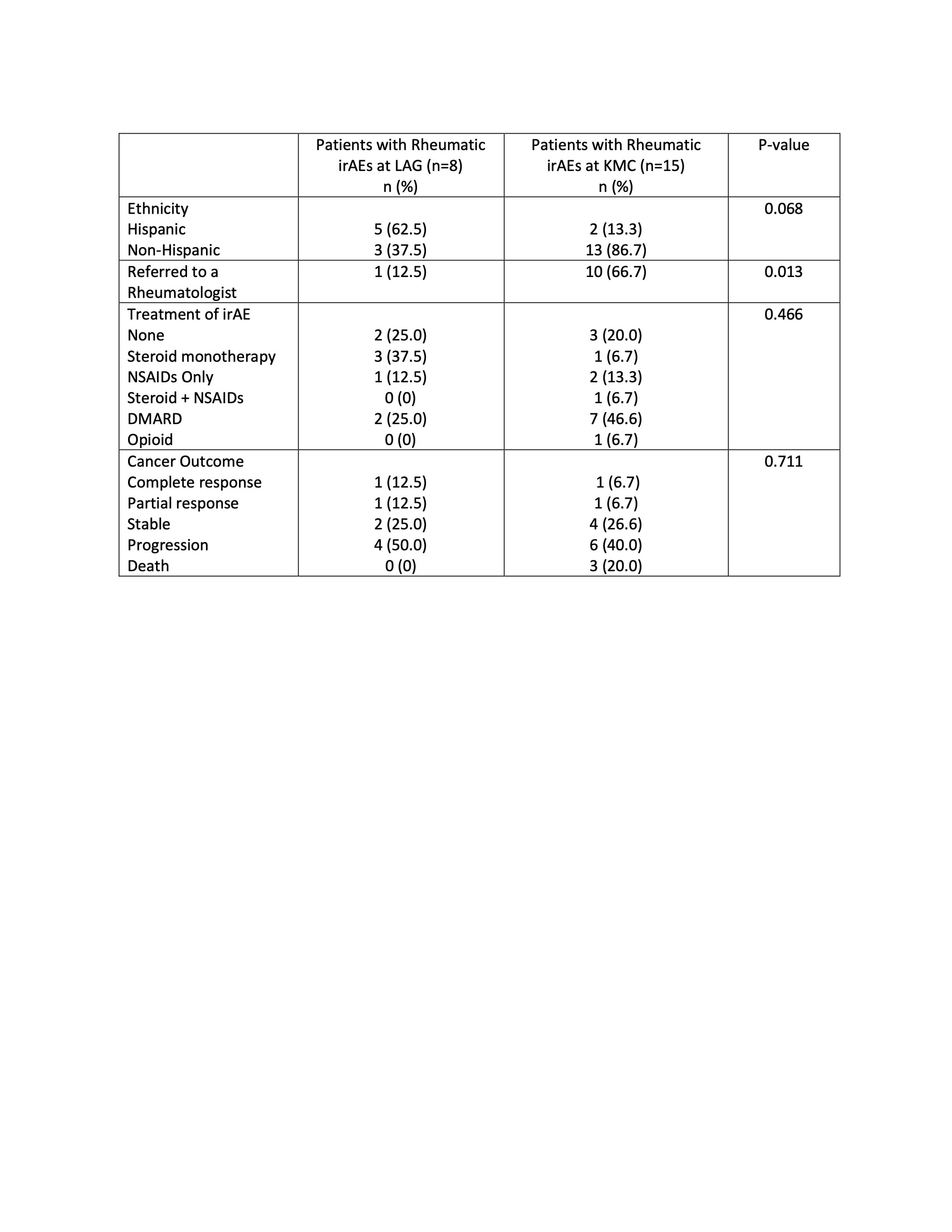
Methods: The electronic medical records of patients 18+ years of age seen at LAG and KMC from May 2015 through May 2021 were screened for treatment with ICIs (nivolumab, pembrolizumab, and/or atezolizumab) by ICD-10 codes, and 613 individual patients (136 at LAG and 477 at KMC) were identified. Of these patients, 30 (22.1%) and 74 (15.5%) developed irAEs at LAG and KMC, respectively. We compared patient demographics, type of iRAEs, and cancer outcomes between the irAE and no-irAE groups at each institution. Among the 30 + 74 patients with irAEs, we identified 23 patients (n=8, 5.9% at LAG; and n=15, 3.1% at KMC) who developed rheumatic irAEs. We compared referral rates to a rheumatologist and management of rheumatic iRAEs between these 2 groups.
Results: No significant differences in demographics and comorbidities were detected between the irAE and no-irAE groups at either institution (Table 1). Across both medical centers, the most common rheumatic irAEs were arthritis (70.0%) followed by myositis (13.0%). Compared to patients at KMC, patients at LAG with rheumatic iRAEs were more likely to be of Hispanic ethnicity (62.5% vs. 13.3%, p=0.068), less likely to be referred to a rheumatologist (12.5% vs. 62.5%, p=0.013) and more likely to be treated with steroid monotherapy for management of rheumatic iRAEs (37.5% vs. 12.5%, p=0.466). There were no significant differences in cancer outcomes between patients with rheumatic iRAEs at each institution (Table 2).
Conclusion: While ICIs have revolutionized therapy for many different types of cancers, they may lead to the development of significant iRAEs, including rheumatic irAEs. To our knowledge, this is the first study to investigate differences in rheumatic irAEs between a public and a private institution located in the same geographic region and staffed by the same group of physicians. The significantly lower rate of referral to rheumatologists among patients with rheumatic irAEs at a public medical center compared to patients at a neighboring private institution raises concern for health care disparities between patients seeking care at a private vs public institution. Studies with larger cohorts of racially and ethnically diverse patient populations are necessary to enhance our understanding of rheumatic irAEs and to ensure equitable care for all patients.
To cite this abstract in AMA style:
Kobashigawa L, Zagelbaum N, Ruddy K, Delgado M, Rai B, Gevorgyan V, Mortezaei K, Stohl W, Taylor-Albert MD E. Rheumatic Immune-Related Adverse Events Following Immune Checkpoint Inhibitor Therapy and Subsequent Referrals to Rheumatologists at a Private vs Public Medical Center in Los Angeles: Ramifications for Health Disparities [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/rheumatic-immune-related-adverse-events-following-immune-checkpoint-inhibitor-therapy-and-subsequent-referrals-to-rheumatologists-at-a-private-vs-public-medical-center-in-los-angeles-ramifications-fo/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatic-immune-related-adverse-events-following-immune-checkpoint-inhibitor-therapy-and-subsequent-referrals-to-rheumatologists-at-a-private-vs-public-medical-center-in-los-angeles-ramifications-fo/