Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Pulmonary arterial hypertension (PAH) is one of the leading causes of mortality in scleroderma-spectrum disorders (SSc). FVC% has been used to differentiate Group 1 (PAH) vs. Group 3 (PH due to chronic lung diseases) in different trials and cohorts. The objective of the current analysis was to assess the relationship between the degree of lung disease on high-resolution computed tomography (HRCT, gold standard) vs. FVC% in identifying those with PH due to Group 1 vs. Group 3 PH.
Methods: In this single center retrospective analysis, 268 patients with SSc who had right heart catheterizations (RHCs) at a tertiary center in US were included. HRCTs were reviewed by 2 thoracic radiologists who assessed the degree of total lung involvement in increments of 10% to up to 30% or > 30% lung involvement, and if there was concomitant emphysema. If emphysema was present, it was classified as mild, moderate, or severe. Chronic lung disease was defined as HRCT showing > 20% total lung involvement due to ILD; or if the total lung involvement due to ILD was 10-20% but the patient had concomitant moderate-to-severe emphysema. Each HRCT was categorized based on FVC% performed closest to the RHC into < 70% or ≥ 70%. Sensitivities and specificities were calculated .
Results: Of 268 RHCs, 57 had Group 1 and 36 had Group 3 PH based on the updated hemodynamic definition of pulmonary hypertension1, as proposed by the 6th World Symposium on Pulmonary Hypertension2. In 75 of 93 patients with Group 1 or 3 PH, we had available HRCT data and 54 were reviewed by thoracic radiologists. Of 75 HRCTs, 34 (45%) patients had moderate-to-severe lung disease (based on the definition above), 20 had mild disease, and 21 did not have any ILD and/or significant emphysema. When we included all HRCTs, FVC% had a sensitivity of 74% (95% CI (59%, 88%)) and specificity of 37% ((95% CI (22%, 51%)) Table 1). When we excluded those with normal HRCTs, FVC% had a sensitivity of 74% (95% CI (59%, 88%)) and specificity of 50% (95% CI (28%, 72%)) when compared to FVC% (Table 2).
Conclusion: FVC% misclassifies a large number of patients into Group 1 vs. Group 3 PH as it may be influenced by other SSc-related disease processes. Future studies should incorporate the degree of HRCT involvement to differentiate between the 2 groups.

Table 1 ACR
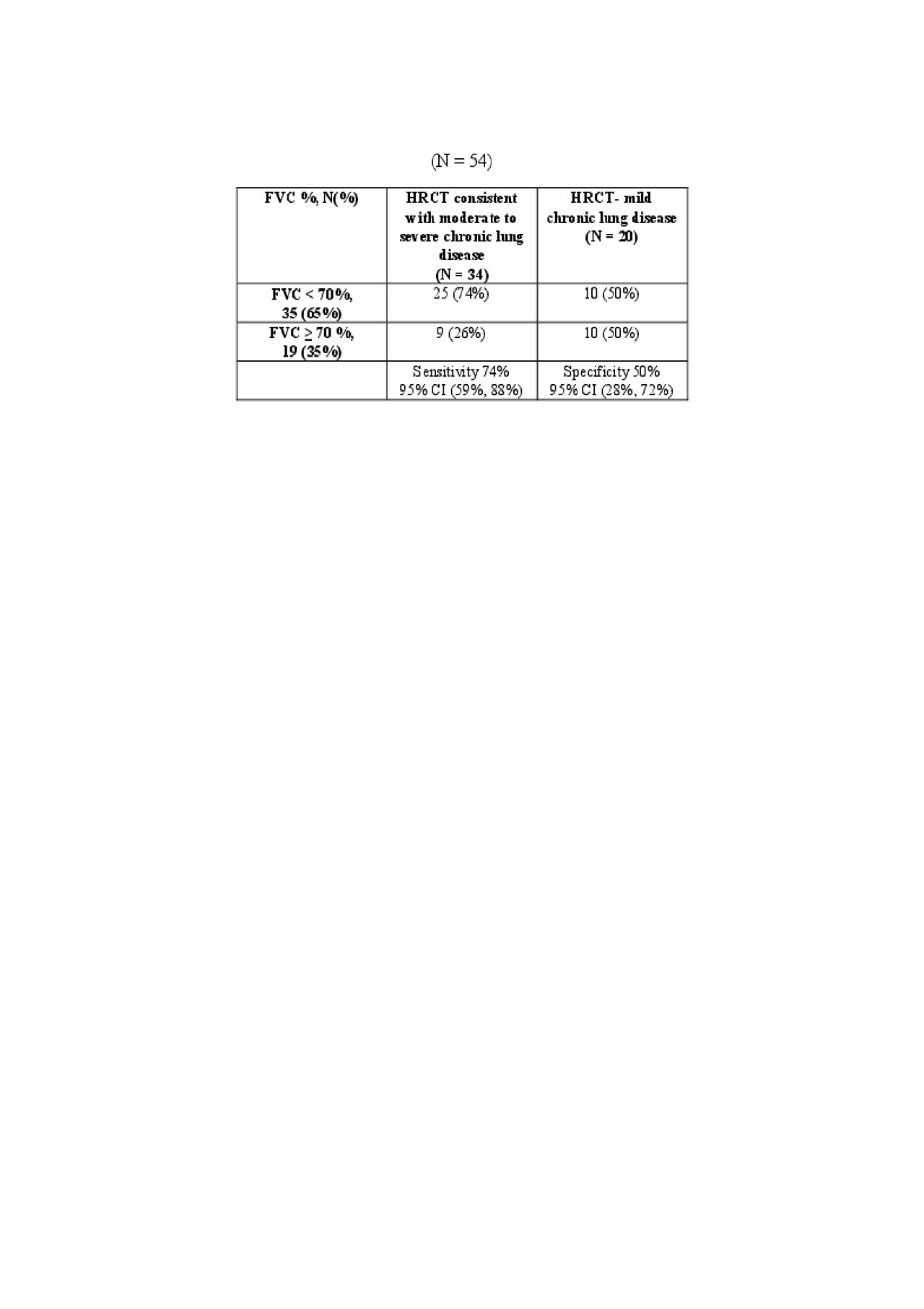
Table 2 ACR
To cite this abstract in AMA style:
Jaafar S, Cronin P, Vummidi D, Visovatti S, Young A, Huang S, McLaughlin V, Khanna D. Relationship Between High-Resolution Computer Tomography and FVC% Predicted for Classification of Pulmonary Hypertension in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/relationship-between-high-resolution-computer-tomography-and-fvc-predicted-for-classification-of-pulmonary-hypertension-in-systemic-sclerosis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relationship-between-high-resolution-computer-tomography-and-fvc-predicted-for-classification-of-pulmonary-hypertension-in-systemic-sclerosis/